Information
on Hodgkin's for Mary Ann
from: Abeloff:
Clinical Oncology, 2nd ed.,
Chapter 90 - Hodgkin's Disease
- Dwight Kaufman
- Dan L. Longo
-
 INCIDENCE
INCIDENCE
-
- About 8,000 cases per year in the United States and 800 cases
per year in Canada
-
- Bimodal age distribution, with peak incidences at 20 to 24
years and 80 to 84 years
-
- Occurs with increased incidence in human immunodeficiency
virus (HIV)-positive persons, but less commonly than do
non-Hodgkin's lymphomas
-
-
DIFFERENTIAL DIAGNOSIS
-
- Diagnosis dependent on identification of the characteristic
malignant cells in an appropriate background of pleomorphic
reactive cellular infiltration that effaces normal nodal
architecture
-
- May be confused with inflammatory lymphadenopathies,
mononucleosis, non-Hodgkin's lymphoma (especially Lennart's and
small lymphocytic), diphenylhydantoin-induced lymphadenopathy,
lymphomatoid papulosis, or nonlymphomatous malignancies
-
- Excisional biopsy of the entire enlarged node essential to
provide the hematopathologist with the best chance to reach the
correct diagnosis
-
- STAGING
EVALUATION
-
- Includes complete history and physical examination, specific
search for B symptoms, hemogram, erythocyte sedimentation rate (ESR),
chemistries,
-
- including lactate dehydrogenase (LDH), chest radiography, and
computed tomography (CT) (if chest radiograph abnormal),
abdominal CT scan, bipedal lymphogram, bilateral bone marrow
biopsies, and aspirates
-
- Staging laparotomy required in patients with clinical early
stage disease only if patient is to be treated with radiation
therapy alone
-
- Post-treatment gallium scan may help distinguish scar from
active residual disease
-
- PRIMARY
THERAPY
-
- Determined by stage of disease: total nodal or subtotal nodal
radiation therapy for early stage, combination chemotherapy for
advanced stage, combined modality therapy for massive
mediastinal disease
-
- Cure in 75 to 80 percent of patients with appropriate
treatment
-
- SALVAGE
THERAPY
-
- Combination of chemotherapy cures nearly two thirds of
patients relapsing after treatment with radiation therapy
-
- High-dose therapy with autologous stem cell transplantation
may result in long-term disease-free survival in 30 to 50
percent of patients who relapse after initial chemotherapy
|
Hodgkin's disease (HD) is a clonal malignancy of the
lymphatic system with protean clinical manifestations. One of the first tumor
types found to be curable at both localized and advanced stages of disease, it
has been of surpassing importance in the evolution of the disciplines of both
medical and radiation oncology. Carefully designed prospective clinical studies
of Hodgkin's disease, with anatomic and pathologic correlations with clinical
outcomes, have led to dramatic improvements in the outlook for patients with
this disease and have served as the template for accurate staging systems and
design of clinical trials leading to improved outlook for other types of cancer
as well. Hodgkin's disease is now cured in about four fifths of the cases, a
near inversion of the odds of mortality as compared with cases diagnosed before
1960. However, many aspects of the biology of Hodgkin's disease remain poorly
understood, and considerable disagreement persists among oncologists regarding
optimal therapy of both early and advanced disease. The debates relate to how
best to achieve an even higher cure rate while minimizing the considerable
treatment-related late side effects of both chemotherapy and radiation therapy.
ETIOLOGY AND EPIDEMIOLOGY
The etiology of Hodgkin's disease has not been
determined. Environmental risk factors do not appear to play
2621
a major role in Hodgkin's disease; however, wood workers, farmers, and meat
workers may be at some increased risk. Hodgkin's disease was one of the first
conditions associated with an HLA allele linkage dysequilibrium, but the
magnitude of the HLA-associated risk is small. The only genetic condition that
appears to predispose to Hodgkin's disease is ataxia telangiectasia, which is
associated with an immunodeficiency syndrome and a predisposition to aggressive
non-Hodgkin's lymphoma as well. However, a role for genetic susceptibility is
suggested by the 99-fold increased risk of Hodgkin's disease in nonaffected
identical twins of Hodgkin's disease patients. [1]
The occasional geographic clusters of cases have suggested the possibility of a
viral etiology with perhaps a long incubation or latent period. No evidence for
a retroviral etiology has been obtained despite an intensive search. [2]
Many cases of coexisting Hodgkin's disease and infectious mononucleosis or of a
diagnosis of Hodgkin's disease in persistently enlarged lymph nodes after
previous involvement with mononucleosis have been reported, leading to
speculation that the Epstein-Barr virus (EBV) may be responsible. [3]
Although a causal role for EBV in the pathogenesis of Hodgkin's disease has not
been proven, recent studies have strengthened the association. [4]
EBV-infected cells in involved nodes have been found in 50 percent of patients
when the sensitive polymerase chain reaction (PCR) was used to detect EBV
sequences. [5]
[6]
The EBV genome as well as EBV-encoded mRNAs are found to be localized in Reed-Sternberg
cells or variants by in situ hybridization or single-cell PCR. [7]
Strong cytoplasmic and membrane expression of EBV-encoded latent gene products
was found in Reed-Sternberg cells in 40 of 84 cases (48 percent) using
immunohistochemical labeling. [8]
In a study of HIV-infected patients with Hodgkin's disease, EBV expression was
detected in 78 percent by immunohistochemistry. [9]
Earlier studies based on case control comparisons using a
surrogate risk group in communities with a high incidence of acquired
immunodeficiency syndrome (AIDS) suggested that HIV infection was not a risk
factor for development of Hodgkin's disease, [10]
[11]
and indeed there has been no easily recognizable epidemic of Hodgkin's disease
in the high-AIDS areas. However, a longitudinal study of 6,700 homosexual men
with known HIV status demonstrated conclusively that the incidence of Hodgkin's
disease in HIV-infected men is increased, with an age-adjusted standardized
morbidity ratio of 5.0, resulting in 19 excess cases of Hodgkin's disease per
100,000 person-years of HIV infection. [12]
In the same population, the relative risk for non-Hodgkin's lymphomas was 37.7
resulting in 225 excess cases per 100,000 person-years of HIV infection.
Hodgkin's disease has not been classified by the Centers for Disease Control as
an AIDS-defining illness, although most of the HIV-infected patients with
Hodgkin's disease would be classified with AIDS on the basis of CD4+ T-cell
count less than 200/mm3 .
Hodgkin's disease represents less than 0.7 percent of all
new cases of cancer in the United States and 0.3 percent of cancer-related
deaths. The age-adjusted incidence rate for Hodgkin's disease is 2.9 per
100,000; this rate has decreased by 15.5 percent over the past 21 years. [13]
This decrease was most significant in the 65 and over age group; however, the
incidence increased modestly in adolescents and young adults ages 15 through 34
years with nodular sclerosis (NSHD) subtype. The apparent decrease in incidence
in the older population is due to improved diagnostic accuracy (cases of
non-Hodgkin's lymphoma having been misclassified as Hodgkin's disease in the
Surveillance, Epidemiology, and End Results [SEER] database from the early
1970s), whereas the increase in NSHD in young adults may be a real increase. [14]
The incidence is higher in whites than in blacks, in males than in females, and
in general, is higher in developed countries than in undeveloped countries. A
bimodal distribution of age at the time of diagnosis is observed with peak
incidences occurring in the 20- to 24- and the 80- to 84-year-old age groups [13]
; the earlier peak predominantly involves patients with diagnosis of NSHD. In
the United States, 7,100 new cases of Hodgkin's disease are estimated for 1998
and 1,400 deaths are expected. [15]
The country-wide age-adjusted death rate declined by 66 percent over the 30-year
period ending in 1989, while the 5-year survival for patients with Hodgkin's
disease increased from 40 percent in 1960-1963 to 78 percent in the 1983-1988
period. For the latest period in which data are available (1989-1993), 5-year
survival is 86 percent
PATHOLOGY
The characteristic neoplastic cells in Hodgkin's disease
generally comprise a small minority of the cellular population of the involved
lymph nodes, existing in a background of normal lymphocytes and inflammatory
cells. In fact, the four histologic subtypes of the Rye classification system,
which has been used almost exclusively in North America since its proposal in
1966, including nodular sclerosis (NSHD), lymphocyte predominant (LPHD), mixed
cellularity (MCHD), and lymphocyte depleted (LDHD), are based entirely on
descriptions of the nonmalignant background of the involved node rather than on
the characteristics of the malignant cells themselves. Recognizing the
increasing role immunophenotyping now plays in the diagnosis of lymphomas,
including Hodgkin's disease, as well as maturing information about the biology,
immunophenotype, and clinical characteristics of the nodular subtype of
lymphocyte predominant Hodgkin's disease (NLPHD), the International Lymphoma
Study Group proposed a revised classification system for Hodgkin's disease in
1994, as part of the Revised European-American Lymphoma (REAL) classification. [16]
The REAL classification system recognizes NLPHD as a distinctly different
disease from classic Hodgkin's disease, which now comprises NSHD, MCHD, and LPHD.
The new World Health Organization (WHO) classification is patterned on the REAL
classification.
A diagnosis of Hodgkin's disease requires microscopic
2622
examination of biopsied specimens, preferably excised lymph nodes. Image-guided
fine-needle aspirates and core biopsies can allow accurate diagnosis of
recurrent or persistent Hodgkin's disease, especially when combined with flow
cytometry; however, excisional biopsy is by the far the most accurate diagnostic
test. Definitive diagnosis of Hodgkin's disease requires (1) identification and
appropriate immunophenotyping of the characteristic neoplastic cells, comprising
the Reed-Sternberg cells and several variants, including lacunar cells,
mononuclear and pleomorphic variants, in "classic" Hodgkin's disease,
and the lymphocyte and histiocyte (L&H), or "popcorn" cells, in
NLPHD; (2) an appropriate background of nonmalignant reactive T lymphocytes,
plasma cells, histiocytes, neutrophils, eosinophils, and stromal cells; and (3)
demonstration of disruption of nodal architecture. The malignant cells
characteristically comprise between 0.03 and 3 percent of the involved tumor
mass in most cases at the time of diagnosis. Cells that are indistinguishable
from classic Reed-Sternberg cells may be seen in several other conditions that
induce adenopathy both inflammatory and malignant, including mononucleosis,
dilantin-induced lymphadenopathy, non-Hodgkin's lymphomas (especially small
lymphocytic lymphoma and Lennert's lymphoma [an ill-defined lymphoma with
clusters of epithelioid histiocytes]), lymphomatoid papulosis, and even melanoma
or carcinomas. Similarly, the cellular background found in a Hodgkin's disease
node may be identical to that seen in a number of nonmalignant, usually
inflammatory lymphadenopathies. Thus, the nodal architecture and the arrangement
of potential Reed-Sternberg cells within a characteristic cellular infiltrate
are all key findings.
Reed-Sternberg Cells
The malignant cell in classic Hodgkin's disease is the
Reed-Sternberg cell or one of its morphologic variants. Reed-Sternberg cells are
giant cells with abundant eosinophilic cytoplasm, and multiple, large, deep
blue-staining nucleoli. The Reed-Sternberg cell characteristically has two or
more nuclei or lobes (it is not entirely clear whether Reed-Sternberg cells are
multinucleated or have polylobated nuclei). The so-called owl's eye appearance
is classic; it is generated by a central nucleolus within each nucleus (or
nuclear lobe). Although nonclassic Reed-Sternberg variants may be diagnostic of
Hodgkin's disease involvement in tissue specimens when the diagnosis has been
previously established, or at relapse, most pathologists require the unequivocal
demonstration of at least one characteristic Reed-Sternberg cell for the initial
diagnosis of classic Hodgkin's disease. Particularly in LDHD, Reed-Sternberg
cells may be quite difficult to distinguish from the cells of other types of
lymphoma, particularly peripheral T-cell lymphoma [17]
[18]
or anaplastic large-cell CD30+ null/T-cell lymphoma. [19]
Lacunar Cell Variant
The lacunar cell variant is characteristic of NSHD. This
cell is a giant cell with multiple nuclei, or a multilobated nucleus, typically
with less conspicuous nucleoli than the classic Reed-Sternberg cell, and a pale,
eosinophilic or clear cytoplasm, if the node is preserved in B5 fixative.
Formalin fixation of the node results in retraction of the cytoplasm around the
nucleus giving the artifactual appearance of a nucleus separated from adjacent
cells by a clear space that is, a nucleus appearing to reside within a lacuna.
These cells are usually quite numerous in NSHD.
A number of immunophenotypic markers are routinely
expressed on Reed-Sternberg cells and its variants in biopsy specimens. However,
their specificity in distinguishing Hodgkin's disease from benign lymphoid
processes or non-Hodgkin's lymphoma has been disappointing. Two moderately
specific antigens, CD30 (Ki-1) [20]
[21]
[22]
[23]
and CD15 (Leu-M1), [21]
are usually expressed on both typical Reed-Sternberg cells and mononuclear
variants found in all subtypes of classic Hodgkin's disease. CD30 (Ki-1) is also
expressed in Ki-1-positive anaplastic large cell lymphoma (ALCL) and can be
expressed on EBV-infected B cells and the Th2 subset of CD4+ T cells. In normal
lymphoid tissue, its expression is restricted to a few extrafollicular activated
T and B lymphoblasts and the B lymphoblasts located at the rim of germinal
centers. [20]
[22]
CD15 (Leu-M1) is present on 85 to 95 percent of normal monocytes and has been
shown to be rarely expressed in immunoblastic lymphomas [24]
and in lymphomatoid papulosis, acute myelogenous leukemia (AML), chronic
myelogenous leukemia (CML), and acute lymphoblastic leukemia (ALL). Other less
specific markers include the low-affinity interleukin-2 (IL-2) receptor (CD25),
transferrin receptor (CD71), and HLA-DR, which are common to activated lymphoid
cells as well as monocytes. Most of the nonmalignant lymphocytes present in
nodes involved with Hodgkin's disease are CD4+ T cells. The paucity of cytotoxic
CD8+ T cells may be related to the absence of class I HLA expression by Reed-Sternberg
cells.
In some cases (about 20 percent), the Reed-Sternberg cell
expresses B-cell markers; in some (about 20 percent), T-cell markers. Rarely
(about 3 percent of cases) the cells express both B- and T-cell markers. In most
cases (about 57 percent), the cells express neither B- nor T-cell markers.
Immunohistologic analysis is difficult because the malignant cells are
surrounded by normal T and B cells and the localization of any particular marker
can be difficult to ascertain with certainty. Examination of DNA extracted from
Hodgkin's disease-involved tissues occasionally shows clonal immunoglobulin gene
rearrangements, clonal T-cell receptor gene rearrangements, both, or neither.
However, this technique is suboptimal for the analysis of genetic changes in
rare cells within a tumor mass. Experiments involving the isolation by
micromanipulation of single Reed-Sternberg cells, too, have yielded some
conflicting results. However, it appears that Reed-Sternberg cells that express
B-cell markers such as CD20 contain clonally rearranged immunoglobulin genes
and, thus, are derived from B cells. Not all cases express B-cell markers, so it
is not clear whether Reed-Sternberg cells can only be derived from B cells. Only
in the LPHD subset do
2623
the malignant cells consistently express lymphoid cell markers (see below).
Lymphocytic-Histiocytic Cell
Lukes originally described a variant cell associated
solely with LPHD, which he called the lymphocytic-histiocytic or L&H cell
variant. [25]
These are large cells with a variable amount of cytoplasm, a multilobated,
puffy, twisted nucleus with a vesicular chromatin pattern, and multiple small,
basophilic nucleoli. Because of their nuclear contour, they have been described
as popcorn cells. L&H cells are usually scattered in faintly defined nodules
composed of small, benign lymphocytes and histiocytes with small clusters of the
malignant cells or may be more abundantly interspersed among diffuse infiltrates
of lymphocytes and epithelioid histiocytes, which completely efface the lymph
node architecture.
Immunophenotyping is key to accurate characterization of
the cells of LPHD. L&H cells are negative for CD15 (Leu-M1), negative or
only weakly positive for CD30 (Ki-1), and almost always positive, in optimally
fixed and processed specimens, for pan-B monoclonal markers such as CD20. [26]
[27]
[28]
[29]
[30]
[31]
[32]
LP popcorn cells also express the B-cell marker CD79a, and in most cases, they
contain J chain, a B-cell component. They express epithelial membrane antigen (EMA),
which is not expressed on any normal B cells. In addition, the non-neoplastic
cells in LP have some interesting features. The T cells that cluster around the
neoplastic cells often express CD57, a natural killer cell marker. Within the
vague nodules of tumor is a meshwork of follicular dendritic cells that express
CD21.
Histologic Subtypes
Classic Hodgkin's Disease
The histologic features of NSHD include the finding of
typical Reed-Sternberg cells, lacunar cells, and interconnective broad sclerotic
bands of collagenous connective tissue that divide the lymph node into cellular
nodules. The lacunar cells may be diffusely scattered or clustered together in
the nodules among a variety of normal cells, lymphocytes, epithelial histiocytes,
eosinophils, and neutrophils. The finding of clusters or sheets of lacunar cells
in an appropriate background in the absence of the sclerotic bands is considered
diagnostic of NSHD in the cellular phase, if diagnostic binucleated or
multinucleated Hodgkin's cells can also be identified. [33]
NSHD disease may be subclassified further into NS lymphocyte predominant, NS
mixed cellularity, and NS lymphocyte depleted, and a two-tiered grading system
is widely used in Europe. However, prognosis among these subtypes is similar
when aggressive treatment, particularly chemotherapy, is used [34]
[35]
; thus, further subtyping of NSHD is of little clinical utility.
NSHD is the most common histologic type occurring in
developed countries, accounting for 50 to 75 percent of all cases. The incidence
of NSHD peaks in late adolescence and the early 20s, but remains the most common
subtype at all ages. A modest female predominance has been reported in most
series. NSHD most frequently involves the mediastinum and the supraclavicular
areas. In the Stanford series reported in 1971, 69 of 85 NSHD cases (81 percent)
had mediastinal involvement and 69 of 76 cases (91 percent) of Hodgkin's disease
with mediastinal involvement had NSHD. [36]
In MCHD, lymph nodes are effaced by a pleiomorphic
cellular infiltrate comprising a mixture of normal histiocytes, neutrophils,
eosinophils, plasma cells, lymphocytes, and fibroblasts, the prototypic
environment referred to as the "appropriate milieu" for the diagnosis
of Hodgkin's disease. The criteria for diagnosis include abundant Reed-Sternberg
cells and diagnostic variants with an absence of fibrotic bands. MCHD accounts
for 15 to 30 percent of all cases of Hodgkin's disease, the second most frequent
histology in non-HIV-infected patients. MCHD is the most frequent histology in
HIV-infected patients, accounting for nearly 60 percent of the cases. There is
peak age incidence between 30 and 45 years, and between ages 40 and 55, MCHD and
NSHD have similar incidences. Male/female ratio is 1.5:1. MCHD is much less
likely than is NSHD to be localized and has a propensity for retroperitoneal
node involvement.
In LDHD, bizarre multinucleated Reed-Sternberg cells
or "malignant-looking" Hodgkin's cells are found in a characteristic
stroma profoundly depleted of lymphocytes and other reactive cells; a
disorganized deposition of proteinaceous fibrillar matrix may be seen. With
modern immunologic techniques, most of the cases previously classified as LDHD
are now identified as belonging to the non-Hodgkin's lymphomas. Fewer than 5
percent of initial Hodgkin's disease diagnoses are classified as LDHD, most
frequently in elderly men presenting with advanced stage disease. LDHD is found
in 20 percent of HIV-infected patients with Hodgkin's disease. It is more
frequently seen as an evolution from MCHD in relapsed, heavily pretreated cases.
LDHD has a propensity for involvement of retroperitoneal nodes and
extralymphatic sites. LDHD can be difficult to distinguish from the
lymphocyte-depleted subtype of NSHD and from non-Hodgkin's lymphoma,
particularly peripheral T-cell lymphoma [17]
[18]
and anaplastic large-cell lymphoma. [19]
In the National Cancer Institute (NCI) series reported by Kant et al., of 39
cases originally diagnosed as LDHD, 11 were reclassified as lymphocyte-depleted
variant of NSHD and 14 others were reclassified as non-Hodgkin's lymphoma. [17]
Lymphocyte-Predominant Hodgkin's Disease
It is now clear that LPHD is a B-cell lymphocytic
malignancy, different both biologically and clinically from classical Hodgkin's
disease. [37]
The diagnosis of LPHD now must meet both histologic and immunophenotypic
criteria. LPHD is characterized by pan B-cell+, CD15-, CD30- neoplastic L&H
cells, which may be sparse or numerous, and abundant lymphocytic and/or
histiocytic stroma with few inflammatory cells and essentially no necrosis. In
most cases, faint nodules can be discerned at low power, and these cases have
been
described as nodular LPHD. A second subtype lacking nodules, diffuse LPHD, has
also been described. Although some cases of diffuse LPHD may be of similar
origin to and possibly evolved from nodular LPHD, the malignant cells of many of
these cases express CD15 and CD30 and lack the characteristic B-cell
immunophenotype. These cases should be reclassified as
"lymphocyte-rich" Hodgkin's disease (see below). [31]
Although clonal immunoglobulin JH gene rearrangements
have not been found, the malignant cells of LPHD are of B-cell lineage. In situ
immunostaining and hybridization techniques demonstrate immunoglobulin light
chain protein and mRNA in the L&H cells of LPHD. [38]
In 28 of 32 cases of LPHD reported by Stein et al., the L&H cells contain
cytoplasmic J chains. [39]
Surface IgM and IgD expression is seen, consistent with a follicular center
origin of these cells; however, rearrangement and expression of the bcl-2
gene typical of follicular B-cell lymphomas is not detected in LPHD, nor is
t(14;18) detected by PCR. [40]
The T cells present in the LPHD-involved nodes are somewhat unusual in that they
express both CD4 and CD57. [41]
LPHD has distinctive clinical features differing from
those of classical Hodgkin's disease. [42]
The incidence is evenly distributed across all ages from 20s to 60s, with a 2:1
male predominance. [43]
Three fourths of cases present as stages I and II, [42]
[44]
[45]
with disease found predominantly in cervical, axillary, or inguinal lymph nodes,
and almost never involving the mediastinum. [46]
There is a very low likelihood of finding intra-abdominal disease at laparotomy
in patients with clinical stage I LPHD presenting in either the inguinofemoral,
cervical, or axillary nodal regions. [44]
This finding implies that these patients can be safely treated with radiation
therapy to only one side of the diaphragm without surgical staging.
Similar to follicular lymphoma, LPHD has a tendency to
run an indolent course, even when left untreated, with an 80 percent 10-year
survival. [43]
LPHD has a very high complete remission rate when treated with radiation
therapy. An analysis of 71 patients with LPHD treated at the Joint Center for
Radiation Therapy in Boston revealed 10-year freedom-from-relapse and 10-year
overall survival rates of 80 percent and 93 percent, respectively. [42]
A distinct tendency towards late relapses, which nevertheless can be effectively
retreated and do not significantly affect overall survival, has been reported.
In one study, initial chemotherapy did not improve the freedom from relapse,
with relapses occurring at a slow but continued rate to at least 10 years after
treatment. [45]
Non-Hodgkin's lymphomas have been reported subsequent to
both treated and untreated LPHD. [32]
[43]
[45]
[47]
Sundeen et al. [47]
described seven cases and Chittal et al. [32]
characterized five additional cases of either evolution from LPHD to diffuse
large cell lymphoma (DLCL) or composite LPHD and DLCL. Both groups considered
the DLCL to have progressed from the LPHD rather than having arisen
independently, although molecular evidence that the subsequent malignant
lymphoma and the LPHD arose from the same cell is lacking. The cases reported by
Sundeen et al. all responded well to therapy, with six of seven complete
remissions and no relapses (with median follow-up of 22 months); the one partial
remission remained stable off therapy for 1.5 years. [47]
Lymphocyte-rich classic Hodgkin's disease is a rare form
of Hodgkin's disease that resembles LPHD, but the malignant cells look like
classic Reed-Sternberg cells rather than popcorn cells. The background contains
small lymphocytes and scattered eosinophils and plasma cells. Recognition of
this form of Hodgkin's disease is felt to be important because this disease
behaves much more like classic Hodgkin's disease than does LPHD
BIOLOGIC CHARACTERISTICS
Attempts to characterize unequivocally the ancestry of
the Hodgkin's neoplastic cell using immunohistochemical or genetic marker
techniques have been inconclusive. Clonal rearrangements of immunoglobulin genes
or T-cell receptor-alpha or -beta genes have been found using Southern blotting
of DNA from involved nodes [48]
[49]
[50]
[51]
; however, in the heterogeneous population consisting of a small fraction of
Reed-Sternberg cells in tissues involved with Hodgkin's disease, these findings
are not readily interpretable. Analyses of the Hodgkin's cell lines show clonal
immunoglobulin rearrangements in six lines, T-cell receptor rearrangements in
four, and none of the cell lines is germline for both. [52]
[53]
[54]
[55]
[56]
Since no Ig protein or T-cell receptors have been detected in any, the observed
Ig and TCR gene rearrangements in cell lines may represent abortive
rearrangements, arrested very early in the stepwise recombinatorial sequence. [55]
These rearrangements are not specific for malignant cells, and since lineage
infidelity may be a common feature of tumors derived from primitive
hematopoietic cells, they may not be used to assign lineage. Thus, although the
available data point to a lymphoid origin, we do not believe them sufficient yet
to justify unequivocal assignment of lymphoid origin to all Hodgkin's cells, and
in fact, a heterogeneous origin is possible.
A search for characteristic marker proto-oncogenes in
Hodgkin's disease, particularly focusing on c- myc, [57]
activating point mutations in c- ras, [58]
and other oncogenes [59]
has been inconclusive. Using the PCR technique, Stetler-Stevenson et al.
reported DNA sequences carrying the fusion of the proto-oncogene bcl-2
with JH Ig sequences, the characteristic finding associated with the t(14;18)
translocation typical of follicular non-Hodgkin's B-cell lymphoma, in 17 of 53
(32 percent) nodal tissues involved with Hodgkin's disease. [60]
The bcl-2 rearrangement was confirmed in one study, with 4 of 21 patients
showing evidence of the translocation [61]
; however, a similar study failed to demonstrate the bcl-2 rearrangement
by PCR analysis in a study of 34 cases of Hodgkin's disease. [62]
It is possible that the bcl-2 translocation may arise in submicroscopic
follicular B-cell lymphoma (composite lymphoma) coexisting
with the Hodgkin's disease, and in fact, three of the cases of Stetler-Stevenson
et al. were found to contain composite lymphoma. [60]
Unlike many other lymphoid neoplasms, no genetic lesion is characteristic of
Hodgkin's disease. The cells are aneuploid and interphase cytogenetics on
numerous single Reed-Sternberg cells from a single mass tends to support the
notion that the cells are clonally derived. Although there is controversy about
the lineage of NS, MC, and LD, many cases express clonally rearranged
immunoglobulin genes that contain point mutations suggesting the possibility
that they are derived from follicular center B cells that have undergone somatic
mutation. Even in cases where the genes are rearranged, immunoglobulin molecules
are generally not detected. Often the messages contain stop codons, deletions,
or frame shifts introduced by mutations that prevent translation. In some cases,
the immunoglobulin genes appear to be polyclonally rearranged, and in some, the
genes are not rearranged.
Genetic lesions affecting many chromosomes and regions
have been identified in Reed-Sternberg cells. None of the many abnormalities
qualify as recurring lesions, and the genes disrupted have not yet been
identified to the extent that putative involvement in pathogenesis can be
inferred. The aneuploidy results in variable numbers of individual chromosomes
being present in the cells. In one study, Reed-Sternberg cells contained between
two and eight copies of individual chromosomes. Mutations in p53 have
been identified in some cases and, depending upon the technique used to examine
the cells, 30 to 60 percent of cases contain evidence of EBV infection. When EBV
is present, it is usually in the form of a clonal episome. Few viral antigens
are expressed, however; LMP1 is the only viral gene product that has been
consistently found in the cases containing EBV genomes.
Many of the characteristic clinical features of
Hodgkin's disease can be explained by expression of cytokines and hematopoietic
growth factors by the malignant cells. [63]
These factors may act in a complex autocrine and paracrine loop, stimulating
both the malignant cells and the nonmalignant stromal cells, including lymphoid
and myeloid cells and fibroblasts, to proliferate and to secrete other growth
factors. These factors could then act locally to stimulate the Hodgkin's cells
or systemically to cause "B" symptoms (fever, night sweats, and weight
loss), immunodeficiency, eosinophilia, thrombocytosis, and marrow fibrosis. Many
known cytokines and growth factors have been found in the supernatants from
various Hodgkin's-derived cell lines. [64]
Expression of a known eosinophil growth factor, IL-5, in the cytoplasm of
clearly identifiable Reed-Sternberg cells was demonstrated in 16 of 16 cases of
Hodgkin's disease with eosinophilia, but in none lacking eosinophilia, by in
situ hybridization of tissue specimens. [65]
Similarly, the Reed-Sternberg cells in involved lymph nodes that were
infiltrated with large numbers of eosinophils were found by immunostaining
techniques to contain and secrete abundant amounts of IgE [66]
; elevated levels of circulating IgE have also been demonstrated in Hodgkin's
disease patients with eosinophilia. Eosinophils express the cell surface Fc
receptor for IgE, the CD23 antigen. The fibrotic bands characteristic of nodular
sclerosis Hodgkin's disease have been postulated to be a response to stimulation
by tumor growth factor-beta (TGF-beta), a cytokine capable of stimulating
proliferation of, as well as collagen synthesis by, fibroblasts. TGF-beta was
demonstrated in the cytoplasm of Reed-Sternberg cells in one case and on the
cell surface of five other cases of NSHD, but in no other histologic subtypes,
by immunohistochemical stain of tumor tissue [67]
; TGF-beta has been found in the urine of four patients with untreated NSHD and
the protein disappeared following effective therapy. [68]
CLINICAL MANIFESTATIONS
The first manifestation of Hodgkin's disease in at least
90 percent of cases is enlarged lymph nodes, with cervical adenopathy the most
frequent presenting site (Table 90-1) . [3]
Although usually painless, pain and tenderness of the enlarged nodes in
Hodgkin's disease may be experienced. Rarely, the pain may be brought on or
exacerbated by alcohol ingestion. Incidental discovery of an asymptomatic
mediastinal mass on routine chest
TABLE 90-1 -- CLINICAL
MANIFESTATIONS OF HODGKIN'S DISEASE
| Findings at presentation |
| Adenopathy |
| Mediastinal mass |
| Splenomegaly |
| Abdominal mass |
| Symptoms |
| Fever, weight loss,
night sweats |
| Pruritis |
| Bone pain |
| Laboratory findings |
| Thrombocytosis |
| Leukocytosis |
| Eosinophilia |
| Elevated
erythrocyte sedimentation rate |
| Elevated alkaline
phosphatase |
| Paraneoplastic syndromes |
| Dermatologic |
| Nodular
prurigo |
| Ichthyosis |
| Psoriasiform
lesions |
| Erythema
nodosum |
| Dermatomyositis |
| Linear
IgA bullous dermatosis |
| Leukocytoclastic
vasculitis |
| Toxic
epidermal necrolysis |
| Renal and metabolic |
| Nephrotic
syndrome |
| Hypercalcemia |
| Hypoglycemia |
| Lactic
acidosis |
| Neurologic |
| Inflammatory
brachial plexopathy |
| Guillain-Barre
syndrome |
| Sensory
ganglionitis |
| Acute
cerebellar degeneraton |
| Stiff-man
syndrome |
| Ophelia
syndrome |
x-ray is not unusual. The most frequent sites of extranodal involvement are, in
decreasing frequency, bone marrow, liver, lung, and pericardium or pleura. If
identified at the time of initial staging evaluation, extranodal involvement
constitutes stage IV disease (with the exception of "E" extranodal
disease, as defined in the Ann Arbor staging classification [69]
). Less frequent sites of extranodal involvement, usually in the setting of
relapsed, far-advanced disease, include skin, bone, and brain.
Constitutional symptoms including high fevers, weight
loss, and drenching and debilitating night sweats have been associated with poor
prognosis. To be defined as "B" symptoms in the Ann Arbor staging
classification, weight loss must be unexplained and greater than 10 percent of
the body weight during the 6 months before staging; fever must be unexplained,
persistent, or recurrent temperatures greater than 38°C over the previous
month; and night sweats must be recurrent and drenching over the previous month.
The pattern of the fever has been noted to be intermittent in some patients, not
occurring daily but in cycles of more or less continuous fever lasting 1 or 2
weeks separated by afebrile periods of similar duration. However, this classic
manifestation of Hodgkin's disease called Pel-Ebstein fever is rare. It is more
common for the fever to peak in the evening and break precipitously in the early
morning hours leading to night sweats. The patient is often unaware of the fever
until it breaks. These systemic symptoms are undoubtedly associated with the
elaboration by the malignant cells of circulating cytokines, such as tumor
necrosis factor (TNF) and IL-1, each of which has been identified in Hodgkin's
cell lines in culture. [70]
The diagnostic work-up for fever of unknown origin may lead to a diagnosis of
Hodgkin's disease, most frequently with the discovery of an abdominal mass by CT
scan or at exploratory laparotomy. [71]
In women, night sweats must be distinguished from "hot flashes"
associated with ovarian failure, particularly in patients previously treated
with chemotherapy.
Laboratory values are frequently completely normal at the
time of diagnosis; the most frequent abnormal findings are hematologic,
including thrombocythemia, eosinophilia, granulocytosis even to the extent of a
leukemoid reaction, elevated ESR, and less frequently, significant anemia.
Elevated ESR is more frequent in more advanced stage disease and may have
prognostic significance in patients treated with radiation therapy alone. The
ESR can be used as a marker for disease recurrence in previously treated
patients. [71]
The serum alkaline phosphatase level is not infrequently elevated in patients
presenting with advanced disease, and can be a signal of either liver
involvement or bone or bone marrow involvement.
In addition to the characteristic systemic symptoms, a
variety of paraneoplastic syndromes have been reported in patients with
Hodgkin's disease, including hematologic manifestations and alterations of the
skin, nervous system, and kidneys. With the exception of thrombocytosis and
eosinophilia, these syndromes are unusual, and are most likely to be seen in
relapsed patients with widespread disease. Eosinophilia occurs in approximately
15 percent of cases [3]
and appears to be related to expression by Reed-Sternberg cells of IL-5, an
eosinophil growth factor. [65]
It can be a manifestation of general leukocytosis or a specific absolute
elevation of eosinophils. A survival advantage has been reported for patients
with selective eosinophilia. [73]
Thrombocytosis is also common, and frequently heralds relapse in patients who
had elevated platelet counts before initial treatment. Both autoimmune
(Coombs'-positive) hemolytic anemia [74]
[75]
[76]
and autoimmune thrombocytopenic purpura (ITP) [77]
can be seen in Hodgkin's disease and, although more likely in advanced disease,
have been reported as presenting manifestations.
Pruritis is a common manifestation of Hodgkin's disease
and may be severe, debilitating, and associated with nodules and plaques. [78]
[79]
It has been reported to precede the diagnosis of Hodgkin's disease by several
years, and the recrudescence of pruritus may be a harbinger of relapse. The
intensity can increase as the disease progresses. A variety of nonspecific
dermatologic disorders can be associated with active Hodgkin's disease, [80]
including ichthyosis and hyperkeratosis, psoriasiform lesions, urticaria,
erythema nodosum, leukocytoclastic vasculitis, [81]
dermatomyositis, [82]
linear IgA bullous dermatosis [83]
[84]
(manifested with widespread, severely pruritic hemorrhagic bullae), and even
fatal toxic epidermal necrolysis. [85]
With the advent of more effective therapy in recent years, it appears that these
skin manifestations are less common than in the first half of the century. The
skin is directly infiltrated with Hodgkin's disease in 0.5 to 3.4 percent of
cases [86]
[87]
either by retrograde lymphatic spread, direct extension from underlying lymph
nodes, or by hematogenous dissemination. Although usually seen in advanced
disease, presentations in the skin as a first manifestation have been reported. [87]
[88]
Renal and metabolic disorders in association with
Hodgkin's disease have been described. A single case of primary renal Hodgkin's
disease has been reported. [89]
Nephrotic syndrome occurring in the absence of amyloidosis or renal vein
thrombosis is an unusual but recognized paraneoplastic syndrome that has been
most frequently reported in Hodgkin's disease, but also in non-Hodgkin's
lymphomas, leukemias, and various carcinomas. [90]
In Hodgkin's disease, the most frequent renal abnormality associated with
nephrotic syndrome is a minimal change lesion or lipoid nephrosis, [91]
[92]
[93]
but membranous and membranoproliferative glomerulonephritides have also been
found. The pathophysiology of these lesions is not known. Secondary systemic
amyloidosis with nephrotic syndrome associated with Hodgkin's disease has been
reported. [94]
Paraneoplastic hypercalcemia has been uncommonly reported in Hodgkin's disease [95]
[96]
; humoral parathyroid hormone (PTH)-like substance has not been found in these
cases. Rather, similar to the hypercalcemia in sarcoidosis and other
granulomatous diseases, the pathophysiology of hypercalcemia in Hodgkin's
disease may be related to increased conversion to 1,25-dihydroxy vitamin D3
, with increased gastrointestinal absorption of calcium. [97]
[98]
Autoimmune hypoglycemia due to antibodies to the insulin receptor has been
reported in three cases of Hodgkin's disease. [99]
[100]
[101]
Finally, a severe case of lactic acidosis in a patient with relapsing Hodgkin's
disease, which resolved with chemotherapy, has been described. [102]
Neurologic complications of Hodgkin's disease include
side effects of therapy, infections, direct effects of tumor, and paraneoplastic
syndromes. Most common is the peripheral neuropathy associated with vincristine
treatment. This is usually initially manifested as loss of Achilles reflexes and
distal numbness and tingling, and can progress to foot drop and difficulty with
fine-motor control of the fingers. An autonomic neuropathy with obstipation is
not infrequent. Vincristine neuropathy is rarely severe before greater than 10
mg cumulative dose, and almost always resolves over several months after the
completion of chemotherapy. Radiation can cause brachial plexopathy or
transverse myelopathy with paraplegia. These irreversible complications are
dose- and fractionation/schedule-dependent and are seldom seen with modern
treatment planning techniques. However, a reversible demyelinating process
affecting the cord may be seen after standard mantle irradiation or other
techniques taking the cord to doses of 40 to 45 Gy. Shock-like sensations along
the spine and tingling and pain in the hands, referred to as Lherrmitte's sign,
associated with neck flexion or arm extension are experienced transiently
starting 2 to 4 months after radiation therapy. [103]
The most common direct complication of Hodgkin's disease is spinal cord
compression by epidural masses originating in vertebrae or in retroperitoneal or
mediastinal lymphatics, by direct extension. [104]
[105]
Hodgkin's disease involves brain parenchyma only rarely, usually as an end-stage
manifestation.
Several debilitating and even fatal paraneoplastic
neurologic syndromes have been reported. [106]
Although the precise pathophysiology of these cases has not been determined, the
cases seem to share an inflammatory component leading to the supposition that
immune phenomena are involved, perhaps cross-reactivity of tumor antigens with
myelin epitopes or normal nerve cell or axonal antigens. Although upper
extremity paresthesias, sensory loss, or weakness in a patient with Hodgkin's
disease should prompt a search for tumor involvement of spinal nerve roots or
brachial plexus and a consideration of radiation-induced brachial plexopathy, a
case of inflammatory paraneoplastic brachial plexopathy associated with
Hodgkin's disease was recently reported. [107]
An acute demyelinating neuropathy resulting in Guillain-Barre syndrome has been
reported in several cases. [108]
[109]
[110]
A fatal case of a rapidly progressing Guillain-Barre-like syndrome in a patient
with recently diagnosed Hodgkin's disease was recently reported. [111]
The patient abruptly developed burning dysesthesias rapidly progressing to
involve total-body pain and sensory loss, autonomic dysfunction with initial
preservation of motor function. The patient died 5 days later. Complete loss of
spinal sensory ganglion cells at multiple levels was demonstrated at autopsy.
Several well-documented cases of subacute or abrupt paraneoplastic cerebellar
degeneration have been reported. [112]
[113]
[114]
Most patients present with ataxia, diplopia, nystagmus, and vertigo. The
neurologic symptoms can be severe and some patients have become bedbound. Both
CT and magnetic resonance imaging (MRI) scans are reported to be normal.
Anti-Purkinje cell antibodies have been found in the sera of some patients.
Effective treatment for Hodgkin's disease has resulted in complete remission of
the cerebellar syndrome. A case of stiff-man syndrome in a patient with
Hodgkin's disease was recently reported. [115]
The patient presented with neuromuscular hyperactivity, painful cramps and
spasms, and limb and truncal stiffness responsive to diazepam. CT scan, MRI,
myelogram, and electroencephalogram (EEG) were normal. Antiglutamic acid
decarboxylase (GAD) cerebellar antibodies were present in the patient's serum.
Effective chemotherapy of the Hodgkin's disease resulted in disappearance of the
symptoms. A psychiatric syndrome characterized by recent memory loss,
depression, personality change, and hallucinations associated with Hodgkin's
disease and termed the "Ophelia syndrome" has been reported. [116]
[117]
In one patient, CT scan, EEG, and cerebrospinal fluid (CSF) studies were normal.
The memory and emotional disturbances improve with successful treatment of the
Hodgkin's disease.
Hodgkin's Disease and HIV
The incidence of Hodgkin's disease is increased among
HIV-infected patients. [12]
Analogous to non-Hodgkin's lymphoma in HIV-infected patients, Hodgkin's disease
has a propensity for presentation with extranodal advanced disease and very
aggressive behavior and is associated with short survival. [9]
[118]
[119]
[120]
[121]
Two thirds of patients present with extranodal disease, with bone marrow
involvement in half, but lung, liver, bone, paraspinal masses, rectum, pleura,
tongue, [122]
and skin [123]
presentations have also been reported. The frequencies of mixed cellularity and
lymphocyte-depleted histologic subtypes are increased and nodular sclerosis
frequency is substantially decreased in comparison with Hodgkin's disease in
non-HIV-infected patients. Only one case of lymphocyte predominance subtype has
been reported. [121]
Patients are susceptible to increased severity of chemotherapy-induced
myelotoxicity, and median survival is less than 12 to 15 months. Nevertheless,
treatment for Hodgkin's disease was successful in patients, particularly those
with a CD4+ cell count higher than 250/mm3 and in
patients without defined AIDS, alowing complete remission and very prolonged
survival in some patients.
STAGING
The Ann Arbor staging system for Hodgkin's disease has
been universally accepted for nearly three decades as the foundation for
reporting and comparing treatment results and for making treatment decisions. [69]
[124]
*From Lister TA, Crowther D, Sutcliffe SB, et al:
Report of a committee convened to discuss the evaluation and staging of patients
with Hodgkin's disease: Cotswolds meeting. J Clin Oncol 7:1630, 1989, with
permission.
Minor refinements have recently been incorporated, recognizing the importance of
technological advances in staging and updated clinical information reported
since the Ann Arbor system was devised [125]
(Table 90-2) (Table Not Available) . For detailed discussions of the evolution
of the staging classifications and for diagrammatic examples of the Ann Arbor
classes, see Kaplan [2]
(pp. 340-365) and a review by Lister and Crowther. [126]
The major modifications include (1) use of CT scanning for detection of
intra-abdominal disease and, when appropriate, delineation of thoracic disease;
(2) a definition of and designation for "bulky" disease; (3) addition
of a post-treatment category for "equivocal" or uncertain complete
remission when residual masses are radiographically detectable but not
pathologically defined; and (4) a clarification of the definition of
"E" extranodal disease.
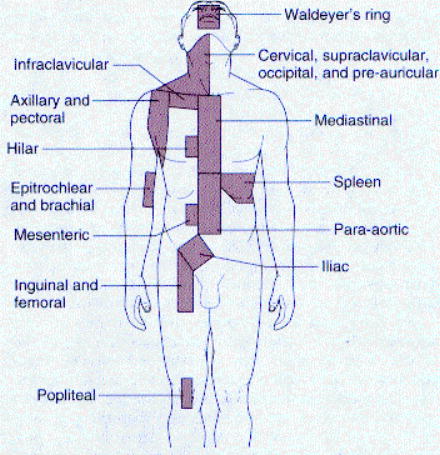
The anatomic lymph node regions (Fig.
90-1) , originally defined by Kaplan and adopted at the Rye Conference, [127]
[128]
used to distinguish stages in the Ann Arbor
 Figure 90-1 Anatomic
lymph node regions. (From Kaplan HS, Rosenberg SA: The treatment of Hodgkin's
disease. Med Clin North Am 50:1591, 1996, with permission.)
Figure 90-1 Anatomic
lymph node regions. (From Kaplan HS, Rosenberg SA: The treatment of Hodgkin's
disease. Med Clin North Am 50:1591, 1996, with permission.)
system are retained in the Cotswolds modification. The term "mediastinal"
was carefully delimited by the Cotswolds committee to include the following
nodal subgroups: (1) prevascular, aortopulmonary; (2) paratracheal, pretracheal,
and subcarinal; and (3) posterior mediastinal. Hilar nodes, internal mammary
nodes, and paravertebral nodes are not in the mediastinal region. Thus, a
thoracic CT scan is necessary to delineate thoracic disease.
In the late 1970s, the poor prognosis associated with
large masses, particularly in the mediastinum, was recognized; this led to the
designation by a subscript "X" to denote large tumor masses in the
revised staging system. Bulky masses in the mediastinum are defined as masses
having a transverse diameter equal to or greater than one third the transverse
diameter of the thorax at T5-T6 on a posteroanterior (PA) chest x-ray. Outside
of the mediastinum, masses greater than 10 cm in diameter are defined as bulky.
The Cotswolds committee attempted to remedy ambiguity in the Ann Arbor
definition of "E" extranodal disease by emphasizing the necessity that
IIE or IIIE be used only to designate a single extranodal site that is either
(1) near and proximal to or (2) in contiguous extension from a site of known
nodal involvement. This distinction is intended to solidify the original
intention that the "E" designation be "for extralymphatic disease
so limited in extent and/or location that it can still be subjected to
definitive treatment by radiotherapy" (Kaplan, [3]
p. 346), which defines a group with the same prognosis, when treated with
radiation therapy, as a group with a similar distribution of nodal-only disease.
Patients with solitary
extranodal-only presentations are classified as stage IE. Patients with more
than one extranodal disease site or with a solitary site not meeting the above
criteria are classified as stage IV. Involvement of liver and bone marrow, even
when apparently solitary and the sole site of identifiable disease, is always
classified as stage IV.
EVALUATION
Pretreatment Evaluation
Most patients with Hodgkin's disease present with
peripheral adenopathy accessible to surgical excision. If possible, an entire
lymph node should be excised for pathologic examination. With a confirmed
diagnosis of Hodgkin's disease, the subsequent evaluation (Table
90-3) includes a medical history, with careful documentation of fevers,
drenching night sweats, weight loss, pruritus, pain elicited by alcohol
consumption, and other changes in the patient's physical state; a complete
physical examination with special attention directed to all lymphatic areas
including Waldeyer's ring (involvement suggests a diagnosis other than Hodgkin's
disease). Perpendicular diameters of nodal masses in each region must be
measured and the size of liver and spleen noted. Laboratory tests should include
complete blood count (CBC), ESR, and complete chemistry panel including
biochemical tests of liver and renal function.
A number of small studies have suggested other serum
markers of prognosis, including soluble CD25, soluble CD30, soluble CD4, soluble
CD8, and certain cytokines such as IL-10. However, none of the studies has
adequately evaluated the degree to which any of these markers are independent
prognostic factors. At the moment, none of these tests is used routinely in
practice. Radiographic evaluation must include PA chest x-ray, CT of the chest
(unless plain chest radiograph is normal), and CT of abdomen and pelvis. Other
noninvasive tests that may be indicated include technetium bone scan,
ultrasonography, and, when pericardial involvement is suspected,
echocardiography. MRI studies usually add little information to the CT scans.
Gallium-67 ( 67 Ga) scanning can occasionally add
useful information for initial staging, detecting unsuspected disease or
confirming disease, [129]
but is most useful in evaluating response to treatment, especially in the
mediastinum. [130]
[131]
[132]
A double-dose (10 mCi) 67 Ga scan with 72-hour delay
in scanning is recommended to re-stage the mediastinum after treatment. The
development of single-photon emission computed tomography (SPECT) 67
Ga scanning [133]
has greatly increased the sensitivity of this procedure. Nevertheless, gallium
scanning is not very useful in initial staging.
Bipedal lymphangiography (LAG) remains a useful staging
procedure, but is used less frequently now than it was in the 1970s and 1980s,
even in referral centers. LAG is the most accurate and sensitive method of
detecting and following retroperitoneal lymph node involvement including the
iliac and para-aortic chains to
TABLE 90-3 -- RECOMMENDATIONS
FOR DIAGNOSTIC EVALUATION OF PATIENTS WITH HODGKIN'S DISEASE
| Mandatory procedures |
| Biopsy, with
interpretation by a qualified pathologist |
| History, with
recording of (1) age; (2) gender; (3) presence or absence of unexplained
fever and its duration; (4) unexplained sweating, especially at night, and
its severity; (5) unexplained loss of weight as a percentage of usual body
weight and rapidity of loss; (6) unexplained pruritis |
| Physical examination
with special attention to evaluation of lymphadenopathy, size of liver and
spleen, and evaluation of bone tenderness |
| Laboratory tests |
| Complete
blood count |
| Erythrocyte
sedimentation rate |
| Liver and
kidney function |
| Alkaline
phosphatase |
| Radiographic
examinations |
| Chest
radiography, posteroanterior and lateral |
| Abdominal
and pelvis computed tomography |
| Bilateral bone marrow
aspirates and biopsies |
| Contingent procedures |
| Thoracic computed
tomography if mediastinal, hilar, and/or mediastinal involvement is seen
or suspected on chest radiography |
| Bipedal
lymphangiogram if available |
| Laparotomy, only if
decisions regarding management will be influenced |
| Liver biopsy (percutaneous
or computed tomography-guided) if there is a clinical or radiographic
indication of hepatic involvement, or if there is evidence of splenic
involvement |
| Optional ancillary procedures |
| Double-dose
gallium-67 scan |
| Technetium bone scan |
| Magnetic resonance
imaging |
| Ultrasonography |
| Echocardiography |
the level of the renal veins, but has little if any utility in evaluating upper
abdominal or mesenteric adenopathy. The characteristic "foaminess"
and/or filling defects can be identified in involved nodes that are too small to
be considered abnormal by CT. The superiority of LAG in detecting para-aortic
node involvement was demonstrated by Castellino et al. in correlations of
lymphographic and CT accuracy with histologic diagnosis after laparotomy. [134]
[135]
[136]
They found an overall accuracy of 95 percent for lymphangiography, with a 3
percent false-positive rate and an 11 percent false-negative rate in predicting
para-aortic lymph node involvement, while the overall accuracy of CT scans for
predicting histologically positive para-aortic lymph nodes was 87 percent, with
a 35 percent false-negative rate. The LAG has the additional advantage of
allowing a cheap and readily available monthly follow-up of response to therapy
and post-therapy follow-up by an abdominal flat plate x-ray (kidney, ureter, and
bladder [KUB]). On the other hand, LAG is tedious and time consuming to perform,
requires 24- and 48-hour follow-up radiographs, and interpretation demands
considerable expertise of the radiologist. Moreover, if chemotherapy is to be
employed, it is no longer of critical importance to detect small sites of
disease not detected by CT. LAG is also associated with a transient decrease in
lung diffusing
capacity; thus, patients with pre-existing interstitial lung disease should
not undergo LAG.
Bilateral posterior iliac crest trephine bone marrow
biopsies should be performed in patients with clinical stage III or IV disease
and those with "B" symptoms. Bone marrow involvement is found in less
than 1 percent of patients stage IA or IIA disease. Peripheral lymph node biopsy
of suspicious nodes on the opposite side of the diaphragm from sites of known
disease should be performed if the result will change the stage. Extralymphatic
sites suspected on the basis of physical examination, radiographic studies, or
laboratory abnormalities of harboring disease, including bone, lung, or liver,
should be biopsied if the results will change the stage or would alter the
treatment plan.
Laparotomy staging to detect subdiaphragmatic disease
in patients with clinical stage (CS) I or II supradiaphragmatic disease is being
done less and less frequently. Staging laparotomy with splenectomy is an
expensive procedure and is associated with potential immediate and delayed
morbidity. Both acute and late bowel and other abdominal complications are seen.
Splenectomy results in a lifelong risk for overwhelming sepsis, notably caused
by encapsulated gram-positive bacteria, most frequently Streptococcus
pneumoniae (pneumococcus). Vaccination 10 to 14 days before splenectomy with
pneumococcal, Haemophilus influenzae, and meningococcal vaccines is quite
effective in preventing these infections. In addition, laparotomy results in 4
to 7 weeks' delay in initiating definitive therapy. [137]
[138]
Thus, laparotomy should be performed only if radiation therapy alone will be
used for pathologically documented early-stage disease. Since chemotherapy is
being used with increasing frequency in early-stage patients, it should be
emphasized that a decision, for whatever clinical reason, to use chemotherapy,
either as sole treatment or in combination with radiation therapy, renders
staging laparotomy unnecessary. Even when radiation therapy is planned as sole
treatment modality for clinical early-stage patients, the utility of staging
laparotomy has been questioned by some. There is now good evidence that
treatment success among clinically staged patients treated with radiation
therapy is not different from that for surgically staged patients, [129]
[139]
[140]
but it must be recognized that the large radiation fields used in these patients
include the intact spleen and portions of the left ventricle and lung, with
potential for increased late toxicity to heart and lung. There are subsets of
patients with supradiaphragmatic CS IA disease with a very low probability, in
some cases approaching zero, of subdiaphragmatic disease. These patients can
clearly be safely treated with radiation therapy alone without laparotomy
staging, in some cases with mantle-field irradiation only. With the above
exceptions, many North American radiation oncologists continue to recommend
surgical staging for CS IA and IIA patients. These issues will be discussed in
greater detail below. Staging laparotomy must be carefully planned among the
surgeon, the pathologist, and the oncologist, and meticulously executed.
The spleen and parasplenic lymph nodes are removed and the spleen is
bread-loafed at 3-mm thicknesses by the pathologist, with careful inspection and
counting of suspicious nodules and histologic examination of all suspicious
nodules and representative specimens of apparent normal spleen. A wedge biopsy
from the right lobe of the liver and needle biopsies from right and left lobes
of the liver are obtained. All radiographically suspicious lymph nodes are
removed, with intraoperative radiographic confirmation of removal of
LAG-positive or equivocal nodes, and samplings from upper and lower para-aortic
nodal chains, porta hepatis, and mesenteric nodes are obtained. Clips should be
placed at the splenic pedicle. Since total nodal radiation including the pelvis
is now used infrequently, oophoropexy during staging laparotomy is of less
importance for young women. Oophoropexy is performed if pelvic radiation therapy
is planned in an effort to spare the ovaries from the harmful effects of
radiation.
Post-treatment Evaluation
The most important initial result of therapy for
Hodgkin's disease is a documented complete remission (CR), the sine qua non of
cure. [141]
One month after completion of the final cycle of chemotherapy or radiation
therapy, all known sites of disease should be re-evaluated radiographically and,
if they are accessible, pathologically. Previously involved bone marrow, liver,
and residual peripheral adenopathy should be biopsied. In general, restaging
thoracotomy or laparotomy is not recommended. Unfortunately, needle aspirates of
residual masses are useful only if they are positive. Persistent but stable
radiographic abnormalities in areas of previous disease that are not accessible
to easy rebiopsy, such as mediastinal widening or persistent distortion of lymph
node architecture on a lymphangiographic study or residual stable masses on CT
scanning, may be classified as CR[U], indicating an unconfirmed or uncertain
remission if the patient is asymptomatic and otherwise without evidence of
active disease. [125]
With modern scanning techniques, a positive post-treatment 67
Ga scan in an area of residual radiographic abnormality, particularly a
mediastinal mass, is very sensitive in detecting residual disease and predicting
relapse. [142]
[143]
[144]
However, a negative 67 Ga scan after therapy has a
significantly lower predictive value. [143]
The sensitivity of MRI scans in distinguishing active residual disease from
fibrosis is not defined.
Patients in CR should be seen at a minimum of 3-month
intervals during the first 2 years following therapy, at 4- to 6-month intervals
during the next 3 years, and yearly after the fifth year. Each visit should
include careful physical examination; laboratory tests including CBC with
differential, ESR, alkaline phosphatase, and liver transaminases; a chest x-ray
if mediastinal disease was present; and KUB if the retroperitoneal nodes remain
radiopaque. Periodic CT scans may sometimes be indicated. On the other hand, a
recent cost-benefit analysis suggests that routine follow-up laboratory and
radiographic tests, other than chest x-ray, rarely led to early detection of
relapse, and method of relapse detection did not have a significant impact on
success of salvage therapy. [145]
Thus, less frequent follow-up is permissible. On the other hand, the late
effects of treatment make it highly desirable to keep in contact with patients
and, as noted below, efforts at early diagnosis of treatment complications
should be made.
THERAPY
Within 5 years of Rontgen's discovery of x-rays,
Hodgkin's disease was first treated with radiation therapy, with dramatic,
although transient, reductions in the size of involved lymph nodes. Radiation
therapy during the first half of the 20th century was delivered with kilovoltage
machines adapted from diagnostic radiology equipment; nevertheless, improvements
were made as a result of increasing doses of radiation, within the limits
allowable by skin toxicity, and extension of radiation fields beyond the limits
of obviously involved lymph nodes. These advances resulted from seminal
observations of the clinical behavior and patterns of relapse of Hodgkin's
disease, initially made by Gilbert in the 1930s, further developed by Peters in
the 1940s and 1950s, to the point that Hodgkin's disease treated in its early
stages with aggressive orthovoltgage radiotherapy could be considered
occasionally curable. The development of the linear accelerator in the 1950s
provided megavoltage therapeutic radiation, thus allowing treatment to large
volumes of disease with decreased skin toxicity. Through a series of randomized
trials beginning in 1962, Kaplan and his colleagues at Stanford University
demonstrated that megavoltage radiation therapy, when delivered to extended
fields and to tumor-sterilizing doses, can cure a majority of patients with
stage I and II disease. [146]
[147]
The careful pathologic and clinical correlations conducted by the Stanford group
expanded and clarified Gilbert's and Peters' early suggestions that Hodgkin's
disease is of unifocal origin and tends to spread in an orderly fashion to
contiguous lymph node groups.
In 1964, the first patient with advanced Hodgkin's
disease was treated at the NCI with MOPP (mechlorethamine, vincristine,
procarbazine, and prednisone) chemotherapy. It became obvious following the
first abstract report of this therapy in 1967 and the subsequent initial full
report in 1970 that even patients with far-advanced Hodgkin's disease could be
cured. Over the past three decades, incremental advances have been made in both
radiation therapy and chemotherapy for Hodgkin's disease, and the two modalities
have been successfully integrated for initial treatment of some presentations.
Because, historically, radiation therapy was the first effective therapy,
attempts to decrease mortality from Hodgkin's disease have frequently involved
the use of more radical radiation therapy including extranodal organs in some
cases. The importance of late toxicity from radiation therapy, especially the
risk of second solid tumors, heart disease, and late
2632
pulmonary toxicity, has only been fully appreciated in the past few years, and
it is now clear that the cumulative risk of dying from the effects of therapy
surpasses the cumulative risk of dying from Hodgkin's disease by 15 to 20 years
from diagnosis. Thus, the trend is now in the opposite direction, and newer
treatment programs are using reduced radiation doses to ever smaller fields,
frequently utilizing chemotherapy to "cure" subclinical disease while
irradiating only the nodal areas known to be involved with disease. The
long-term effects of these programs will not be known for many years. It is a
truism, but should not be forgotten, that susceptibility to dying two decades
after diagnosis from a late toxicity of treatment requires first and foremost
that the patient be cured of Hodgkin's disease by the initial treatment. Even
large gains in decreasing late treatment-related mortality at the expense of
modest decreases in initial efficacy may have a net negative survival impact.
In 1999, most oncologists still agree that the preferred
treatment of most cases of early-stage Hodgkin's disease is radiation therapy,
that the preferred treatment of advanced-stage disease is combination
chemotherapy, and that optimal treatment of bulky disease, regardless of stage,
is combined chemotherapy and radiation therapy. Disagreements persist regarding
the location of the boundary between early and advanced stage; furthermore,
there are proponents of combined-modality therapy for both nonbulky early-stage
and some cases of advanced stage disease, [148]
as well as proponents of the routine use of chemotherapy alone for early-stage
disease. [149]
Radiation Therapy
Randomized trials from Stanford and elsewhere comparing
involved field (IF) with successively larger treatment fields, including
subtotal nodal (STNI) and total nodal irradiation (TNI), plus radiation to
extranodal organs at risk, demonstrated improved freedom from relapse (but not
improved overall survival, as discussed below), with more extensive fields. [147]
These studies led to the development of the following principles of curative
radiation for Hodgkin's disease:
- Patients must be carefully and accurately staged, in most cases including
laparotomy and splenectomy, if radiation is to be used as sole treatment.
- Treatment must include, in addition to the areas of known involvement,
"prophylactic" treatment to extended fields including all nodal
areas likely to be subclinically involved. [124]
- Techniques to ensure dose homogeneity and appropriate organ shielding must
be employed, including (a) individualized, or custom-tailored, radiation
therapy portals, (b) large treatment portals, and (c) equally weighted
opposed AP portals.
Based on retrospective evaluation of kilovoltage
treatment data from Peters, [150]
Kaplan concluded that cure requires a tumor dose of 40 to 44 Gy to clinically
and subclinically involved nodal areas, [151]
doses that could not be practically delivered until the development of the
linear accelerator. Based on analysis of dose-response data from the megavoltage
era, most radiation oncologists now believe these doses to be unnecessarily
high, especially to nonbulky and subclinical areas. [152]
Furthermore, as will be discussed in more detail below, recent treatment
programs are de-emphasizing surgical staging as well as extended field
radiotherapy for treatment of early-stage disease.
The techniques of radiation therapy for pathologic stage
(PS) I and IIA Hodgkin's disease have been reviewed in considerable detail, [3]
[147]
[153]
[154]
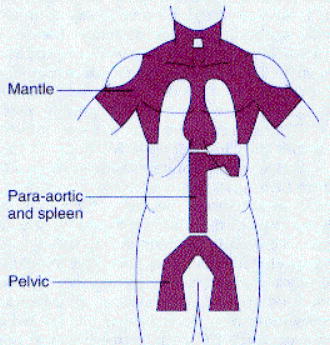
and will only be discussed in general terms here. "Standard" treatment
fields for pathologically staged supradiaphragmatic disease is mantle and para-aortic
fields plus splenic pedicle, referred to as STNI (Fig. 90-2)
. A unilateral preauricular field is added for patients with preauricular
involvement or with high cervical involvement. In addition, Waldeyer's ring is
treated for patients with bulky high cervical involvement. There are some
"favorable" subsets of patients with PS IA and IIA disease, discussed
further below, who can be safely treated with mantle field irradiation alone.
Treatment of CS II disease and most cases of CS I disease with radiation therapy
alone requires irradiation of the entire spleen volume. Patients thus treated
are rendered functionally asplenic, with the same long-term risks encountered by
splenectomized patients; in addition, the apex of the left ventricle and the
base of the left lung receive considerable scatter radiation dose.
Most patients with subdiaphragmatic stage I and II
disease are treated to para-aortic/splenic pedicle fields plus pelvis fields,
with the iliac and inguinal regions treated with an "inverted Y," as
demonstrated in Figure 90-2 . When the patient is
clinically staged, the spleen must be irradiated. Patients presenting with CS I
inguinal and/or femoral adenopathy can be treated with inverted
 Figure 90-2 Total nodal
irradiation of the mantle, spade, and inverted Y fields. (From Kaplan HS:
Hodgkin's Disease, 2nd ed. Cambridge, Harvard University Press, 1980, with
permission.)
Figure 90-2 Total nodal
irradiation of the mantle, spade, and inverted Y fields. (From Kaplan HS:
Hodgkin's Disease, 2nd ed. Cambridge, Harvard University Press, 1980, with
permission.)
Y alone, if CT and lymphangiogram demonstrate no disease in the iliac nodal
regions. Patients with PS III1 A, if treated with
radiation alone, require irradiation of mantle, para-aortic, and splenic pedicle
fields, plus inverted Y, referred to as total nodal irradiation (TNI). Most
oncologists today do not consider PS III1 A disease as
"early" stage, and offer chemotherapy alone, obviating the necessity
for TNI. An understanding of the potential complications of radiotherapy is as
important for the medical oncologist as it is for the radiation oncologist. The
thyroid, lungs, heart, intestines, and spinal cord are most frequently affected
by long-term, or chronic, toxicity. Toxicities to lungs and heart can be
potentiated by chemotherapy drugs that also have cardiac and/or pulmonary
toxicity, particularly doxorubicin and bleomycin. A 3.2-fold increased risk for
fatal myocardial infarction following mantle field irradiation has also been
reported. [155]
[156]
Although it has been maintained that the risk of cardiac and pulmonary
complications is largely associated with obsolete radiation techniques, data
from Stanford University comparing patients treated in the pre-1972 era with
those treated in the post-1982 era suggest that these complications persist
despite the use of newer therapeutic techniques. With increasing follow-up time,
radiation-induced solid tumors have replaced leukemia as the most commonly
observed second malignancies, with cumulative incidence of 10 to 13 percent at
15 years. The risk for solid tumors, especially lung cancer and breast cancer,
increases steadily with time, and constitutes the major cause of excess
mortality after 10 years. In children, radiation therapy results in premature
closure of epiphyses of growing long bones and immediate cessation of further
growth. Finally, although gonads can frequently be shielded, direct or scatter
radiation to a total dose greater than 200 cGy can result in sterility in males
and, depending on age at treatment, ovarian failure and sterility in women
receiving 200 to 1,000 cGy to the ovaries.
Chemotherapy
There are several excellent chemotherapy regimens now
available, each with apparently similar anticancer efficacy if delivered in
optimal doses and schedules, but with considerable differences in patterns of
both early and late toxicity. Both the oncologist's familiarity with a regimen
and a consideration of the potential toxicities should enter into the decision
of which regimen to choose. Despite advances in salvage therapy for relapsed
Hodgkin's disease, we believe that the best opportunity a patient has of being
cured is afforded by the initial treatment regimen, and any modification of that
regimen for any reason other than as necessitated by severe toxicity already
manifested may deprive the patient of a chance for cure, and is thus
indefensible. We have thus formulated a set of principles that we believe are
broadly applicable to the use of any chemotherapeutic regimen that has
legitimate claim to being potentially curative for Hodgkin's disease [157]
:
- Do not modify planned doses or schedules of chemotherapy in anticipation
of toxicity that has not yet happened, nor for short-term,
non-life-threatening toxicity, such as emesis. Although the ability to
deliver full doses can be compromised by the patient's intolerance of the
drugs' toxicities, which in turn may be influenced by age and other
variables associated with poor prognosis, every effort should be made to
deliver maximum tolerated doses.
- Consider dose escalation of the myelotoxic agents in subsequent cycle for
patients who experience minimal neutrophil (i.e., no granulocyte count below
1,500/mm3 ) and platelet (i.e., no platelet count
below 100,000/mm3 ) nadirs in the first cycle of
chemotherapy.
- In order to identify slow responders or nonresponders, reassess tumor
status with each cycle of chemotherapy with a careful physical exam, a chest
radiograph for patients with thoracic disease, and a KUB for those with
abnormal lymphangiograms. Tumor progression at any time during treatment
should prompt switching to a non-cross-resistant regimen, with plans to
proceed to high-dose salvage therapy if possible.
- Although a minimum of six cycles of all currently used chemotherapy
regimens is believed to be necessary, slow responders may require more than
six. We recommend treating for two additional cycles following a complete
remission or after identification of stable, nonresponding residual masses,
usually to a maximum of eight cycles. In our experience, six cycles of
therapy has been sufficient in 85 percent of patients and 15 percent have
required eight cycles. Thus, complete noninvasive reassessment of all sites
of disease after four cycles of chemotherapy is required for comparison with
the studies obtained after the sixth cycle. There seems little justification
for treating with the same regimen for greater than eight cycles. [157]
Additional cycles beyond eight for patients with residual tumor masses that
seem to be shrinking when reassessed after the eighth cycle are either
futile or unnecessary (though it may not be possible at the time to discern
which) and will only increase morbidity without
added benefit, and may delay switching to a more effective therapy for those
patients with active residual disease.
- Residual masses following treatment, whether stable for two cycles or
still seemingly responding, require careful assessment. This may consist of
biopsy, gallium scanning, [142]
[143]
or watchful waiting with radiographic reassessment at frequent intervals.
Evidence of disease activity will prompt alternative therapy, either
radiation therapy to residual masses, conventional dose salvage
chemotherapy, or high-dose therapy with stem-cell rescue.
MOPP and Derivatives
MOPP (Table 90-4) was the
first successful combination drug regimen for the treatment of Hodgkin's
disease. The regimen was designed on the principles of combining drugs with
independent antitumor activity and nonoverlapping organ toxicity, delivery of
all drugs in full therapeutic dose with a fixed schedule of administration and a
sliding scale of dose adjustment based on marrow toxicity, and cyclic delivery
to allow normal tissue recovery. The results of long-time follow-up of 188
patients treated at the NCI with MOPP between 1964 and 1976 was updated in 1986 [159]
[160]
[161]
: overall CR rate was 84 percent (stage II, 100 percent CR; stage III, 82
percent CR; stage IV, 77 percent CR; no B symptoms, 100 percent CR; with B
symptoms, 78 percent CR). The overall survival was 48 percent at 19 years,
virtually plateaued since the 10th year of follow-up, and the 15-year
disease-free survival of the overall cohort was 54 percent. Patients free of
Hodgkin's disease comprised 30 percent of the deaths (30 of 98). Thus, the
majority of these patients with far-advanced disease and B symptoms were cured
of Hodgkin's disease.
Similar success with the MOPP regimen was subsequently
reported by several other groups, [162]
[163]
[164]
and MOPP rapidly became the accepted treatment for advanced-stage Hodgkin's
disease. The impact of MOPP and subsequent multidrug regimens on the outlook for
Hodgkin's disease has been dramatic. In the first 20
TABLE 90-4 -- CHEMOTHERAPY
REGIMENS FOR INITIAL TREATMENT OF HODGKIN'S DISEASE: REGIMENS FOR ADVANCED
DISEASE
| DRUGS |
DOSE |
SCHEDULE |
CYCLE LENGTH |
COMMENTS |
| MOPP |
|
|
|
|
Nitrogen mustard
Vincristine
Procarbazine
Prednisone |
6 mg/m2
1.4 mg/m2 (no cap)
100 mg/m2
40 mg/m2 |
IV days 1 & 8
IV days 1 & 8
PO days 1-14
PO days 1-14 |
4 wk |
6 cycles min
8 cycles max |
| MVPP |
|
|
6 wk |
6 cycles |
Nitrogen mustard
Vinblastine
Procarbazine
Prednisolone |
6 mg/m2
6 mg/m2
100 mg/m2
40 mg |
IV days 1 & 8
IV days 1 & 8
PO days 1-15
PO days 1-15 |
|
|
| ChlVPP |
|
|
|
|
Chlorambucil
Vinblastine
Procarbazine
Prednisolone |
6 mg/m2
(10 mg max)
6 mg/m2 (10 mg max)
100 mg/m2
40 mg |
PO days 1-14
IV days 1 & 8
PO days 1-14
PO days 1-14 |
4 wk |
6 cycles min |
| ABVD |
|
|
|
|
Doxorubicin
Bleomycin
Vinblastine
|
25 mg/m2
10 U/m2
6 mg/m2
375 mg/m2 |
IV days 1 & 15
IV days 1 & 15
IV days 1 & 15
IV days 1 & 15 |
4 wk |
6 cycles min |
| Alternating MOPP/ABVD |
|
|
|
4-wk MOPP cycle alternating with
4-wk ABVD cycle |
| MOPP/ABV hybrid |
|
|
4 wk |
8 cycles total |
Nitrogen mustard
Vincristine
Procarbazine
Doxorubicin
Vinblastine
Vincristine
Bleomycin |
6 mg/m2
1.4 mg/m2 (max 2.0 mg)
100 mg/m2
40 mg/m2
35 mg/m2
6 mg/m2
10 U/m2 |
IV day 1
IV day 1
PO days 1-7
PO days 1-14
IV day 8
IV day 8
IV day 8 |
|
Reassess after 6
cycles
If CR, 2 more cycles
If PR, give involved field radiation to residual disease,
then 2 more cycles chemo |
| MA/MA hybrid |
|
|
4 wk |
6-8 cycles, then involved field
XRT to residual disease |
Nitrogen mustard
Vincristine
Procarbazine
Prednisone
Doxorubicin
Vinblastine
Bleomycin
Decarbazine |
6 mg/m2
1.4 mg/m2 (max 2.0 mg)
100 mg/m2
40 mg/m2
35 mg/m2
6 mg/m2
10 U/m2
375 mg/m2 |
IV day 1
IV day 1
PO days 1-7
PO days 1-7
IV day 15
IV day 15
IV day 15
IV day 15 |
|
|
years after the introduction of MOPP, the age-adjusted mortality in the United
States from Hodgkin's disease decreased from 1.8 to 0.7 per 100,000, [164]
while the 5-year survival rate doubled from 40 percent in 1960 to 82 percent in
1993. [15]
Unfortunately, toxicity of MOPP proved to be significant.
Long-term toxicities of MOPP include sterility and secondary myeloid
malignancies, including acute myeloid leukemia and myelodysplastic syndrome.
Virtually all men are rendered permanently azoospermic following six cycles of
MOPP and over half of women over 26 years old become amenorrheic. Thirteen cases
of acute leukemia and two cases of aplastic anemia were observed in the NCI
series. No cases of leukemia occurred later than 9 years after the completion of
therapy and all cases but one occurred in patients who received radiation
therapy in addition to MOPP. Many reports have confirmed increased risk for
myeloid malignancies occurring 2 to 10 years after treatment with MOPP or other
alkylator-based regimens, with a risk of 2 to 10 percent at 10 years. The risk
returns to that of the normal population by 10 years after therapy. Radiation
therapy adds to the risk of myeloid leukemia in relation to the size of the
fields. Total or subtotal nodal radiation approximately doubles the leukemia
risk when added to chemotherapy; small field radiation therapy appears to add
little to the risk. The risk for both sterility and myeloid malignancies is
related to the cumulative dose of alkylator and procarbazine. The lifetime risk
of acute leukemia and myelodysplasia from MOPP alone is 2 to 3 percent.
The acute toxicities include reversible bone marrow
suppression in nearly all patients, nausea and vomiting, and largely preventable
but painful phlebitis at the site of intravenous injection of nitrogen mustard.
Peripheral or autonomic neuropathies from vincristine, manifested by
paresthesias, weakness, foot drop, and obstipation, are dose-related, but are
usually not debilitating. Vincristine neuropathy is usually completely
reversible. In the 1970s, the late toxicities of MOPP (i.e., sterility and
myelogenous leukemia/myelodysplastic syndromes) were only little appreciated,
and the primary focus of many clinical researchers was on decreasing the rate of
acute toxicities to MOPP, which were perceived to be the main drawback to
routine use of the regimen. It should be emphasized that the limiting acute
toxicities of the 1970s may be minor annoyances or less in the era of indwelling
catheters and ports, hematopoietic growth factors, and serotonin 5-HT3 receptor
antagonist antiemetics.
Many groups introduced modifications of the MOPP
program by addition, deletion, or substitution of one or more drugs, yielding
alkylator-based regimens that were felt to be easier to tolerate and/or to
deliver. Of these MOPP derivatives, MVPP and ChlVPP (chlorambucil, vinblastine,
procarbazine, and prednisone) have become the most widely used. MVPP (nitrogen
mustard 6 mg/m2 , with vinblastine 6 mg/m2
substituted for vincristine, and prednisolone used in all six cycles, with
cycles lengthened from 4 to 6 weeks) [166]
[167]
[168]
[169]
affords CR rates and relapse-free rates similar to those of MOPP and is
associated with only insignificant neurotoxicity; emesis is comparable to and
marrow toxicity worse than with MOPP. The ChlVPP regimen was developed as a
largely oral regimen with fewer short-term side effects than are seen with
either MOPP or MVPP. [170]
Oral chlorambucil was substituted for nitrogen mustard in the MVPP regimen in
order to decrease vomiting and the risk of nitrogen mustard-associated
phlebitis, and a shorter cycle length of 28 days was used. Extensive experience,
both in England [171]
[172]
[173]
[174]
and in the United States, [175]
has shown that ChlVPP possesses efficacy comparable to that of MOPP. The results
of ChlVPP in 960 patients with early and advanced disease has recently been
summarized. [176]
Although acute toxicities are indeed substantially lower than with MOPP, the
frequency of both sterility and secondary myeloid malignancies following ChlVPP
is similar to that following MOPP.
In summary, 80 percent of patients with advanced-stage
Hodgkin's disease with constitutional symptoms treated with MOPP or one of its
alkylator-based variants can be expected to enter complete remission; of these,
one third will relapse. Since about one third of the patients who relapse can be
salvaged, approximately two thirds of advanced-stage patients with symptoms will
be cured. The long-term results are influenced by the tumor burden and
accompanying constitutional symptoms, age, and performance status. All of these
regimens are associated with a high rate of gonadal damage, and the risks of
second myeloid malignancies are approximately the same as with MOPP.
Several retrospective studies have suggested adverse
prognostic consequences of decreased dose intensity of one or more of the agents
in the MOPP regimen. [161]
[177]
[178]
[179]
[180]
[181]
[182]
[183]
[184]
[185]
It is probable that similar dose-response relationships hold for other regimens
as well, and we remain emphatic in recommending that dose modifications of
protocol doses be made only for toxicities already experienced, using sliding
scale modifications as recommended by the designers.
ABVD and Hybrid Regimens
The ABVD (doxorubicin, bleomycin, vinblastine, and
dacarbazine) regimen (Table 90-4) was designed as a
non-cross-resistant regimen for the treatment of patients relapsing after
treatment with MOPP, and was initially shown to be effective in this setting. [186]
[187]
[188]
ABVD was then combined in alternating cycles with MOPP for previously untreated
patients with advanced disease in trials beginning in 1974; although ABVD alone
was not prospectively evaluated in untreated patients for several years
thereafter, it has now become clear that ABVD is an effective regimen for
initial treatment of advanced Hodgkin's disease, and in many settings it may be
the preferred regimen. By contrast, it is not terribly effective when used as
salvage therapy for MOPP-resistant patients. It has a different spectrum of
toxicities from the alkylator-based regimens, with virtually no gonadal toxicity
or risk for myeloid malignancies. Both acute and long-term pulmonary toxicity
due to bleomycin are not infrequent and may be severe;
there is also an increased risk of anthracycline-associated cardiac damage.
Unfortunately, there are no reports of long-term follow-up for late toxicities
in substantial numbers of patients treated with ABVD alone.
Several mature randomized comparisons of MOPP or related
regimens with ABVD or combinations of MOPP and ABVD (either with cycles of MOPP
alternating with cycles of ABVD or hybrid regimens in which all or most of the
drugs of both regimens are delivered in each 4-week treatment cycle) have now
been reported. Comparison between 12 cycles of MOPP versus six cycles of MOPP
alternating with six cycles of ABVD in stage IV Hodgkin's disease was begun in
1974 in Milan, and updated 10-year results have been reported. [189]
[190]
[191]
Complete remission rates were 74 percent and 89 percent; the relapse-free
survivals were 46 percent and 68 percent; and the 10-year overall survival rates
were 58 percent and 69 percent for MOPP and the MOPP-ABVD alternating regimens,
respectively. The differences between the relapse-free survivals reached
statistical significance favoring MOPP-ABVD, but the differences in overall
survival were not significant. An Eastern Cooperative Oncology Group (ECOG)
study confirmed the effectiveness of alternating cycles of MOPP and ABVD in a
comparison with BCVPP (carmustine, cyclophosphamide, vinblastine, procarbazine,
and prednisone). [192]
A European Organization for Research in Cancer Therapy (EORTC) trial in stage
IIIB and IV compared eight cycles of MOPP with two cycles MOPP alternating with
two cycles of ABVD for a total of four 2-month cycles of both regimens. [193]
Radiation therapy was given to sites of residual disease for patients with
partial responses. Surprisingly low CR rates were observed in both arms (57
percent vs. 59 percent) and no significant differences were seen in relapse-free
survival or overall survival.
A Cancer and Acute Leukemia Group B (CALGB) study
reported in 1992 allows more detailed analysis of these regimens [194]
: 361 patients with stage III and IV Hodgkin's disease or relapsing after
previous radiation therapy were randomized among 12 cycles of alternating
MOPP-ABVD, MOPP alone, and ABVD alone (the four-drug regimens were given for six
to eight cycles). The CR rates for both ABVD and MOPP-ABVD were significantly
higher than the CR rate for MOPP alone: 67 percent for MOPP, 82 percent for ABVD,
and 83 percent for MOPP-ABVD ( P = 0.006 for MOPP vs. the other
regimens). Significant differences were also observed between the failure-free
survivals (FFS) measured at 5 years: 50 percent for MOPP, 61 percent for ABVD,
and 65 percent for MOPP-ABVD ( P = 0.02). On the other hand, the
differences between the overall survivals (66 percent, 73 percent, and 75
percent for MOPP, ABVD, and MOPP-ABVD, respectively) were not significant.
Subset analysis suggested that the significant difference in FFS between MOPP
and the two ABVD-containing regimens could be accounted for entirely by a subset
of older patients with two or more extranodal sites of disease (43 percent vs.
62 percent FFS for MOPP and ABVD, respectively). The FFS rates in a low-risk
group (<50 years with stage III or stage IV with only one extranodal site)
were similar with the three regimens. MOPP was reported to cause substantially
greater acute myelotoxicity than did ABVD, particularly in older patients, which
resulted in progressive dose reductions and treatment delays in patients treated
with MOPP. Only 24 percent of all patients received at least 85 percent of the
planned dose of nitrogen mustard by the final cycle, whereas doxorubicin was
delivered in near full doses to most patients receiving ABVD. Of serious concern
was the 3 percent fatality rate from pulmonary complications on the ABVD arm.
The risk of death from ABVD is thus similar to the risk of death from MOPP.
Two regimens were designed to overcome ab initio tumor
cell resistance, utilizing the assumptions of the Goldie-Coldman mathematical
model of tumor cell resistance, which predicted that a hybrid regimen using all
the drugs in two effective and non-cross-resistant regimens in each and every
cycle (i.e., use of all of the effective drugs in a single cycle) would minimize
emergence of resistant clones. [195]
[196]
The Milan group's hybrid regimen, termed "MA/MA," consisted of a
half-cycle of MOPP on Day 1 and a half-cycle of ABVD on Day 15 of each 28-day
cycle. [190]
[197]
[198]
The Vancouver MOPP-ABV hybrid regimen differs from MA/MA in that (1) the highly
emetogenic agent dacarbazine was eliminated, (2) the dose of doxorubicin was
increased from 25 to 35 mg/m2 per cycle, (3) the ABV
portion is given on Day 8 instead of Day 15, and (4) eight cycles are given
instead of six, with involved field radiation therapy administered to sites of
residual disease after six cycles of chemotherapy. [158]
[199]
[200]
[201]
An uncontrolled trial of this regimen in 170 previously untreated patients with
advanced Hodgkin's disease suggested that this regimen is similar to both ABVD
and alternating MOPP-ABVD in efficacy. [201]
The complete remission rate was 84 percent, the projected 7-year overall
survival was 80 percent, and the projected 7-year FFS was 65 percent. A
comparison of both sequences of MOPP and ABVD MA/MA hybrid versus alternating
MOPP/ABVD was conducted by NCI-Milan. [198]
Patients with stages IB, bulky IIA, IIB, IIIA and B, and IV were randomized.
Radiation therapy was given following chemotherapy to sites of pretreatment
bulky disease. No significant differences in CR rate (91 percent vs. 89
percent), 10-year FFP (67 percent vs. 69 percent), or 10-year overall survival
(74 percent vs. 72 percent) between alternating MOPP/ABVD and MA/MA hybrid were
detected. Similarly, a large trial conducted by NCI-Canada comparing MOPP/ABV
hybrid with alternating MOPP/ABVD in 301 patients with stage IIIB or IV
Hodgkin's disease and patients relapsed after previous wide-field irradiation
detected no differences in CR rate, 5-year FFS, or 5-year overall survival
between the two regimens. [202]
An Intergroup trial comparing MOPP-ABV hybrid with ABVD alone demonstrated
insignificant differences in CR rates, FFS, and overall survival. [203]
These three trials suggest that ABVD, MA/MA hybrid, MOPP/ABV hybrid, and
alternating MOPP-ABVD are essentially equivalent in treatment efficacy. It would
further appear from these trials that Goldie-Coldman predictions have not led to
the development of a more effective therapy in Hodgkin's
disease. A separate Intergroup trial of MOPP/ABV hybrid versus MOPP times six
cycles followed by ABVD times three cycles showed a small but statistically
significant improvement CR rate, 8-year FFS, and overall survival at 8 years for
MOPP/ABV over sequential MOPP times six followed by ABVD times three. [204]
The latter regimen does not test Goldie-Coldman principles, and should be
expected a priori to be very little different from MOPP alone in either short-
or long-term results.
As expected, long-term toxicities following MOPP or ABVD
are substantially different. The gonadal toxicity and risk for myeloid leukemia
subsequent to MOPP therapy are significant and discussed in greater detail
below. In contrast, ABVD alone results in only transient germ-cell toxicity in
most males [204]
[205]
[206]
[207]
[208]
and the alternating regimen MOPP/ABVD appears also to result in about half the
incidence of sterility seen with MOPP. [207]
The incidence of second myeloid malignancy after ABVD is virtually nil, as
previously noted; in fact, only four cases have been reported in patients
receiving ABVD alone. Although AML/myelodysplasia would be expected to be lower
in patients treated with MOPP/ABV than with MOPP alone because of the lower
exposure to nitrogen mustard and procarbazine, six cases among patients treated
with the hybrid regimen were reported in the first Intergroup trial of MOPP/ABV
versus ABVD. [203]
In fact, this trial was terminated early by the Data Safety and Monitoring
Committee because of excessive toxicity in the MOPP/ABV arm, with significant
increases in life-threatening or lethal neutropenia, thrombocytopenia,
infection, pulmonary toxicity, and second malignancies.
In all clinical trials of ABVD, significant and sometimes
life-threatening acute pulmonary toxicity is reported. In the CALGB study, [194]
[209]
ABVD was associated with acute fatal pulmonary toxicity in four patients, two
late lung carcinomas, and fatal cardiac failure in one patient in complete
remission, accounting for 7 of the 12 deaths in patients without evidence of
Hodgkin's disease. It would be anticipated that alternating MOPP/ABVD or hybrid
MOPP/ABV would be associated with less pulmonary toxicity than ABVD, since
cumulative doses of bleomycin are lower. However, as noted above, in the
Intergroup trial of MOPP/ABV versus ABVD, pulmonary toxicity was greater in the
MOPP/ABV arm. The problem of synergistic heart and lung toxicity in patients
treated with both ABVD and radiation therapy is likely to be much more serious,
but has yet to be fully defined.
Summary
MOPP and most of the MOPP-derived alkylator-containing
regimens, such as ChlVPP or MVPP, are effective therapy for advanced Hodgkin's
disease, and cure the majority of patients when delivered in optimal therapeutic
doses (i.e., doses at the maximum tolerable levels, as defined by the observed
toxicity in each individual patient without ad hoc dose modifications). Gonadal
toxicity and induction of secondary myeloid malignancy are expected to be
similar for all alkylator-containing regimens. Controlled trials in advanced
Hodgkin's disease have demonstrated that ABVD, alternating MOPP/ABVD, MA/MA
hybrid, and MOPP/ABV hybrid regimens are virtually equal in therapeutic
efficacy. All four ABV(D)-containing regimens have fairly consistently been
shown to give modestly improved CR rates and freedom-from-relapse rates in
comparison with MOPP alone, with modest or statistically insignificant
improvements in overall survival. The advantage of the ABV(D)-containing
regimens over MOPP appears to be limited to patients older than 50 years of age.
It must be noted that in each of the randomized trials, MOPP dosing has been
systematically attenuated from the originally reported NCI regimen, in a manner
expected to reduce efficacy.
Both early and late toxicities of ABVD are different
from the toxicities of MOPP. The myeloid toxicity of ABVD appears to be more
tolerable, especially in older patients, than that of MOPP, allowing less dose
modification. Neither gonadal toxicity nor the risk for second leukemias is
significant following ABVD. On the other hand, morbidity and mortality from
cardiac and pulmonary toxicities of doxorubicin and bleomycin, respectively,
particularly when mediastinal radiation therapy is used, may be substantial. As
has been noted, 15- to 20-year follow-up data are necessary to appreciate fully
the late toxicities of any regimen, data that have unfortunately not been
reported for patients treated with ABVD alone. Since late toxicities are related
to cumulative doses of the offending drugs, the seven- or eight-drug regimens
appear to mitigate each of the principal toxicities associated with both MOPP
and ABVD, while exposing the patient to some potential risk for all of them. It
is unclear at this time where the balance lies, but it appears that, based
largely on the toxicity profile, ABVD may have an overall edge as an initial
treatment of choice for most patients with advanced Hodgkin's disease. Clearly,
if combined-modality therapy including mantle field irradiation is planned,
alternating MOPP-ABVD or MOPP-ABV hybrid is preferable to ABVD, since cumulative
doses of bleomycin and doxorubicin are lower and interactive toxicities between
the drugs and radiation therapy would likely be less frequent and/or less
severe.
Therapy for Specific Presentations
Supradiaphragmatic Stages I and II
Radiation therapy
Radiation therapy is generally considered the preferred
therapy for most patients with stage IA and IIA supradiaphragmatic Hodgkin's
disease. [146]
[210]
[211]
[212]
[213]
[214]
[215]
The radiation therapy techniques for treatment of PS I to II disease developed
at Stanford, and widely adapted in North America and elsewhere, are summarized
in Table 90-5 . [147]
Patients with supradiaphragmatic PS IA and IIA are treated with subtotal
lymphoid irradiation (STLI); whereas TLI has been used for patients with
"B" symptoms. When patients are treated in this manner, complete
remission rates approaching 100 percent are expected,
TABLE 90-5 -- CHEMOTHERAPY
REGIMENS FOR INITIAL TREATMENT OF HODGKIN'S DISEASE: REGIMENS COMBINED WITH
RADIATION
| DRUGS |
DOSE |
SCHEDULE |
CYCLE LENGTH |
COMMENTS |
| VBM |
|
|
4 wk |
6 cycles, then involved field
radiation |
Vinblastine
Bleomycin
Methotrexate |
6 mg/m2
10 U/m2
30 mg/m2 |
IV days 1 & 8
IV days 1 & 8
IV days 1 & 8 |
|
|
| Stanford V |
|
|
4 wk |
3 cycles (12 wk), then 36 Gy
radiation to sites of initial tumor bulk >5 cm |
Doxorubicin
Vinblastine
Nitrogen mustard
Vincristine
Bleomycin
Etoposide
Prednisone |
25 mg/m2
6 mg/m2
6 mg/m2
1.4 mg/m2 (2.0 mg max)
5 U/m2
60 mg/m2
40 mg/m2 |
IV days 1 & 15
IV days 1 & 15
IV day 1
IV days 8 & 22
IV days 8 & 22
IV days 15 & 16
PO qod |
|
|
| NOVP |
|
|
3 wk |
3 cycles, then involved field
radiation |
Mitoxantrone
Vincristine
Vinblastine
Prednisolone |
10 mg/m2
1.4 mg/m2
6 mg/m2
100 mg |
IV day 1
IV day 8
IV day 1
PO days 1-5 |
|
|
with 15 to 30 percent relapse rates and overall survival at 10 years ranging
between 80 and 95 percent, depending upon stage. Results of 109 PS I to II
patients, including those with massive mediastinal involvement, treated at
Stanford with radiation therapy alone, with a median follow-up of 6 years, are
shown in Table 90-6 . [213]
These results remain the gold standard for comparison of therapy for early-stage
Hodgkin's disease. Nevertheless, there has been a significant shift away from
these techniques over the past decade, and much of the earlier dogma regarding
radiation dosing and field size and necessity for staging laparotomy has now
been abandoned. Analyses of radiation dose-response curves for patients treated
with modern techniques have suggested a plateau above 3,600 cGy, allowing
decreased total doses with no apparent adverse effect. Recently, the
International Hodgkin's Disease Collaborative Group has published results of a
meta-analysis of randomized trials comparing less versus
TABLE 90-6 -- RADIATION
TECHNIQUES FOR PS I-II: STANFORD APPROACH *
| Dose |
| 40-44 Gy in 4-6 wk
by opposed fields to each field |
| STLI fields |
| Mantle plus splenic
pedicle and para-aortics to just below iliac bifurcation
("spade" field) |
| Hila treated to
full dose, even when uninvolved |
| Shields for larynx,
spinal cord, humeral heads, and heart |
| Two-week break
between mantle and subdiaphragmatic fields |
| TLI fields |
| Also includes
iliacs (inverted Y) |
| Special characteristics |
| High cervical
disease: preauricular region and Waldeyer's ring treated to 3,600-4,400
cGy |
| Hilum involved:
ipsilateral lung irradiated to 1,600 cGy with thin lung blocks over 4 wk |
| Abbreviations: STLI,
subtotal lymphoid irradiation; TLI, total lymphoid irradiation. |
*Data from Hoppe RT: Radiation therapy in the
management of Hodgkin's disease. Semin Oncol 17:704, 1990.
more extensive radiation fields in early-stage patients. [216]
Eight trials with greater than 10 years' follow-up involving 1,974 patients were
analyzed. Recently updated individual patient data were available for all of the
patients randomized in these trials. The meta-analysis showed that more
extensive radiotherapy reduced the risk of treatment failure (either resistant
or recurrent disease) from 43.4 percent to 31.3 percent at 10 years,
approximately a one-third improvement. However, there was no improvement in
overall 10-year survival, 77.0 percent and 77.1 percent, respectively, for more
versus less. This is because salvage chemotherapy was successful in curing most
of the patients who failed radiation. Finally, staging laparotomy is recommended
with decreasing frequency, and is omitted entirely by many centers, including,
since 1988, the Stanford University group.
Although the staging laparotomy is being used with
decreasing frequency, the lessons about the clinical course of Hodgkin's disease
taught by the practice of meticulous surgical staging must not be forgotten.
Abdominal CT scanning has only about 50 percent accuracy in predicting splenic
involvement. [135]
[136]
One third of patients with enlarged or abnormal-appearing spleens are found at
splenectomy to have no splenic involvement and, conversely, about one third of
patients without CT abnormalities in the spleen or elsewhere below the diaphragm
will be upstaged by laparotomy. There are prognostic factors in a subset of CS
IA patients that predict an acceptably low likelihood (i.e., <10 percent) of
finding subdiaphragmatic disease. [217]
[218]
These groups include (1) all women with CS IA, (2) men with nonbulky mediastinal
disease, (3) men with lymphocyte-predominant histology, and (4) men with
cervical disease above the hyoid bone. Limited radiation therapy without staging
laparotomy and without chemotherapy can be recommended for these patients. The
remaining men with CS IA disease and all patients with CS IIA (80 percent of all
CS I to II patients) have approximately 30 to 40 percent risk of
occult subdiaphragmatic disease. These patients have traditionally required
pathologic staging to authenticate early stage before proceeding with definitive
radiation. Either the addition of chemotherapy to radiation therapy or treatment
with chemotherapy alone obviates the necessity for laparotomy. Surgical staging
allows for selection of patients to receive radiation therapy alone, reduces the
subsequent need for salvage chemotherapy, and may allow smaller radiation
treatment fields. The absence of the spleen allows the use of smaller
subdiaphragmatic treatment fields and significant reduction in the volume of
abdominal tissue irradiated, with significant decrease in radiation exposure to
the left kidney, the left ventricle, and the lower left lung field. In Europe
and elsewhere, many early-stage patients are treated without laparotomy with
extended field radiation (TNI or TLI) including splenic radiation. [139]
[140]
[219]
Overall survival has not yet been reported to be compromised with this approach,
in part due to the effectiveness of salvage chemotherapy, but possibly also due
to the short overall follow-up times in these studies.
Certain prognostic factors have been reported to predict
an increased probability of relapse after treatment with radiation therapy
alone. Most significant of these have been the presence of bulky masses and
constitutional symptoms. An analysis of 180 patients with PS IB and IIB disease
treated at Stanford and at the Joint Center for Radiation Therapy revealed that
in these symptomatic patients, the most significant adverse characteristic at
initial presentation was the presence of both fevers and weight loss. [220]
Patients with both fevers and weight loss had a 52 percent 7-year relapse rate
and only 57 percent 7-year actuarial survival, which was worse than for patients
with massive mediastinal disease treated with radiation therapy. The relapse
rate for patients with fever only was 31 percent, and was 19 percent for
patients with weight loss only. The presence of night sweats was not an adverse
prognostic factor. Patients with PS IB or IIB disease on the basis of night
sweats only had the same freedom-from-relapse rates and survivals as patients
with PS IA or IIA disease, respectively, and the presence of night sweats in
addition to either fever or weight loss or both did not worsen the prognoses
compared with similar patients lacking night sweats. Prognostic factors reported
in other studies, [221]
[222]
but not confirmed by the analysis of the combined Stanford-Joint Center cohorts,
included gender (male is worse), histologic subtype, number of sites of
involvement, and the presence of extranodal disease. Clearly, tumor burden is
the most important adverse factor, [223]
and most prognostic indicators serve as surrogate markers for tumor bulk. Age
has only modest influence on relapse rate but has a significant influence on
survival, due to decreased effectiveness of salvage therapy in the older age
group. [212]
[221]
Combined-modality therapy
About 40 percent of the remainder of clinical early-stage
patients (i.e., all patients with CS II disease and men with CS I lacking the
above favorable characteristics) will have occult disease below the diaphragm.
Whether or not pathologic staging is necessary in these patients is the key
question driving many recent trials in early stage disease. Recent studies have
focused on the treatment of clinically staged patients with radiation therapy
alone, chemotherapy alone, or combined-modality therapy. More than 20 randomized
trials comparing radiation therapy with combined chemotherapy plus radiation
therapy have been conducted. Although improvements in relapse rates in
early-stage patients treated with combined-modality therapy are easily
demonstrable, no trial has yet shown superior survival for combined-modality
therapy in patients with PS I and II disease, even among subsets with adverse
prognostic features at presentation, as compared with radiation therapy alone. [138]
[213]
[224]
[225]
[226]
A meta-analysis of 23 reports with 2,999 early-stage patients did not
demonstrate survival differences between patients treated with extended field
radiation and those treated with combined-modality therapy. [210]
Nevertheless, many clinicians still believe that avoidance of relapse should be
paramount and continue to recommend combined-modality therapy, in part to avoid
the psychological trauma for patients who relapse and must then be treated with
salvage therapy. There would be little controversy about this practice were it
not for the additive, or even synergistic, toxicity of radiation and most
chemotherapy regimens currently known to be effective, including the possibly
increased risk of secondary myeloid malignancy with alkylator-based regimens and
the cardiac and pulmonary toxicities associated with doxorubicin and bleomycin.
Several strategies have been explored in efforts to
circumvent the late toxicities observed following extended field radiation
combined with chemotherapy, including programs utilizing smaller radiation
treatment fields, lower radiation doses, and less toxic chemotherapy regimens.
Included in the latter are programs utilizing decreased numbers of cycles of
standard chemotherapy regimens and less aggressive
2640
chemotherapy regimens developed specifically for combined-modality programs. The
Stanford group developed the VBM regimen (vinblastine, bleomycin, and
methotrexate) as an adjunct to radiation therapy in combined-modality programs,
and now omits staging laparotomy in all patients. VBM is said to have no gonadal
toxicity, limited leukemogenicity, and no cardiac toxicity, although its
toxicities, especially neurologic toxicity due to vinblastine, mucositis, and
pulmonary toxicity, have been reported to be major problems. [146]
A randomized trial comparing subtotal or total lymphoid irradiation (STLI/TLI)
versus VBM for two cycles followed by involved field radiation therapy, followed
by four additional cycles of VBM was conducted in patients with CS IA and IIA
(plus a small number of patients with night sweats as the only B symptom). [227]
With median follow-up greater than 4 years, results were equivalent, with 92
percent FFP for STLI versus 87 percent FFP for VBM plus involved field radiation
therapy. Other groups have confirmed the efficacy of VBM plus regional
radiation, but hematologic, neurologic, and pulmonary toxicities were limiting. [228]
[229]
The Stanford group uses a more intense chemotherapy regimen, Stanford V, for
combined-modality treatment of patients with bulky and/or advanced stage
Hodgkin's disease. [230]
Another approach to reducing the toxicity of
combined-modality therapy is to deliver only modest doses of involved field
radiation therapy (15 to 30 Gy) following full courses of combination
chemotherapy. This approach has proved effective in children, in whom avoidance
of both splenectomy and high-dose radiation therapy to growing bones is
mandatory because of the risks of postsplenectomy sepsis and cessation of bone
growth, respectively. [231]
[232]
Furthermore, with their longer overall survival, children treated with radiation
therapy have a greater cumulative risk of second solid tumors. However, it has
not been shown that radiation therapy is necessary in either children or adults
treated with effective chemotherapy. Recently the Pediatric Oncology Group (POG)
has shown conclusively that low-dose radiation does not improve the results in
children with stages IIB through IV disease following alternating MOPP-ABVD. [233]
In summary, combined-modality therapy has not been shown
to be superior to radiation therapy alone in early-stage patients, nor has it
been demonstrated to be superior to chemotherapy alone in advanced-stage
patients, except those with bulky tumor masses. [234]
Advocates of combined-modality therapy in adults cite data largely from
uncontrolled trials [148]
[235]
[236]
or from flawed randomized studies [237]
in advanced Hodgkin's disease to suggest superior results. We have cautioned
against the routine use of this practice outside the clinical trial setting in
advanced-stage patients because of the risk of second cancers and fatal heart
attacks associated with radiation therapy. [234]
Chemotherapy alone in early stage HD
A chemotherapy-only approach to the treatment of
early-stage Hodgkin's disease avoids both staging laparotomy and the toxicities
of combined-modality therapy. Since chemotherapy is more effective in treating
low-bulk than high-bulk disease in advanced-stage patients, it would seem
unlikely a priori that it would be less effective in early-stage than in
advanced Hodgkin's disease, or that optimal results in early-stage disease
require even more intensive therapy (i.e., combined-modality therapy) than is
required to cure advancedstage disease. Chemotherapy is effective in children
with early-stage disease [174]
[238]
[239]
and has been shown in several randomized trials to be equivalent to
combined-modality therapy in adults with stage I to IIIA disease. [167]
[240]
[241]
Two prospective randomized trials have compared
chemotherapy alone with radiation therapy alone for early-stage adult patients. [242]
[243]
[244]
Both studies randomly assigned surgically staged patients to receive either six
cycles of MOPP chemotherapy or standard radiation therapy to mantle and para-aortic
fields. However, the trials differed in their inclusion criteria for
randomization, and have come to different conclusions. At the NCI, 110 patients
with central PS IA and IB (thoracic and abdominal only), IIA, IIB, and PS III1
A were randomized between MOPP and STLI. [149]
[242]
Patients with peripheral IA (disease above the clavicles or below the inguinal
ligament) were treated with radiation therapy, either to a minimantle or an
inverted Y, without randomization. After the trial was begun, it became clear
that radiation therapy alone was inappropriate therapy for patients with massive
mediastinal disease and patients with PS III1 A
disease; these patients were not entered after the first 5 years of patient
accrual. The CR rates were 96 percent for both approaches. When all randomized
patients were analyzed, statistically significant improvements in both 17-year
disease-free survival (85 percent vs. 64 percent) and overall survival at 17
years (93 percent vs. 76 percent) were seen for MOPP as compared with radiation.
When these results were reanalyzed after exclusion of seven patients with
massive mediastinal disease and 13 patients with PS III1
A who had been randomized in the early years of the trial and who fared very
poorly with radiation alone (leaving 86 randomized patients, of whom 79 were
stage II), there was no difference in overall survival and a small but
statistically insignificant advantage in disease-free survival (DFS) for
patients treated with MOPP. From this analysis, we conclude that MOPP and
radiation therapy afford equivalent DFS and overall survivals, at least for
stage IIA and IIB patients. Since only seven patients with PS I were randomized,
it is difficult to draw firm conclusions for these patients, although we believe
it unlikely that they would fare less well with chemotherapy than do stage II
patients.
In the Italian trial, all patients with PS IA and IIA
were randomized between MOPP and extended field radiation therapy; patients with
B symptoms were excluded. [244]
The authors concluded that radiation therapy was superior. Both the CR rates and
relapse rates were similar in the two arms; however, significantly better
overall survival (93 percent vs. 56 percent at 8 years' median follow-up) was
found in the patients randomized to radiation therapy. The poor survival in the
MOPP-treated cohort resulted from a significantly lower salvage rate among
patients who relapsed: only 2 of 12 (17 percent) of the relapsed MOPP-treated
patients achieved second CR compared with 10 of 12 (83 percent) second CRs among
the relapsed patients in the radiation therapy arm. The 30 percent relapse rate,
the 22 percent 1-year relapse rate, and the low second CR rate are substantially
worse than was observed in the MOPP arm in the NCI trial, which included a
greater proportion of relatively more advanced patients, including patients with
B symptoms. This result thus seems to us to be substantially worse than should
be expected for optimally delivered chemotherapy in a minimal-disease situation,
and in fact approximates the expected result for MOPP-treated patients with
stage IVB disease. Based on the results of the NCI trial, we believe that at
least for stage II patients, chemotherapy should constitute an acceptable
primary treatment alternative to radiation therapy. While more data are needed
in stage I patients, it is unlikely that radiation alone will be inherently
inferior to chemotherapy in this group. Other regimens, including ABVD or
MOPP-ABV hybrid, would appear to have some advantages in toxicity profile over
MOPP, particularly for young patients for whom fertility is a consideration. A
small pilot study of ABVD in clinically staged stage I and II patients has been
reported. [244]
With very short median follow-up duration and small numbers of patients, the
projected progression-free and overall survival rates at 42 months were 84
percent and 95 percent, respectively.
Subdiaphragmatic Stage I or II
Subdiaphragmatic stage I and II Hodgkin's disease
accounts for only 3 to 4 percent of all new cases of Hodgkin's disease. Eighty
percent of these patients present with groin adenopathy (inguinal, femoral, or
superficial iliac) and the remainder will present with disease confined to the
abdomen. [71]
[246]
[247]
[248]
[249]
[250]
[251]
[252]
[253]
[254]
[255]
[256]
Patients presenting with abdominal Hodgkin's disease tend to be older, more
likely to be male, and more likely to present with constitutional symptoms than
those with either peripheral subdiaphragmatic or supradiaphragmatic
presentations; mixed cellularity histology is more common among central
abdominal presentations than are the other histologies. [248]
[249]
In a series of 473 patients of all stages from Stanford, four patients presented
with fever of unknown origin and were found to have an abdominal mass that
proved to be Hodgkin's disease. [70]
Patients may also present with lower extremity edema due to lymphatic or venous
obstruction. Hodgkin's disease has been diagnosed at splenectomy after
presentations with splenomegaly, splenic rupture, or apparent splenic abscess.
Extranodal small bowel, stomach, or large bowel presentations are quite rare.
Initial diagnosis of intra-abdominal disease will
frequently be made at exploratory laparotomy; however, when the diagnosis is
secure and abdominal disease is known to be present, laparotomy to define extent
of abdominal disease would appear to contribute little additional information.
For patients with femoral, inguinal, or superficial iliac presentations,
abdominal CT scans and bipedal lymphangiography is adequate staging; staging
laparotomy for peripheral subdiaphragmatic presentations would appear to have
limited value, since treatment will usually not be altered by the results. A
review of 76 patients with CS IA to IIB Hodgkin's disease with inguinal
presentations who had staging laparotomies showed that laparotomy resulted in a
change in stage in one third, but a clinically important upstaging to PS III or
IV occurred in only 5 percent. [249]
Only one of 21 patients with CS IA groin presentations with negative
lymphangiograms was found at laparotomy to have disease outside the true pelvis
(splenic involvement) and another was found to have a positive iliac node. Of 55
patients with CS IB, IIA, or IIB, six were down-staged from CS IIA to PS IA,
three were upstaged to IVA on the basis of liver disease, and one was upstaged
to IIIA (after a blind scalene biopsy). Splenic involvement was found in 28
percent.
Evaluation of treatment in these patients is difficult
because of the small numbers and the variability in treatment strategies. Most
patients reported in the literature have been treated with extended field
subdiaphragmatic radiation therapy fields or total nodal radiation therapy with
or without adjuvant chemotherapy. It appears from subset analysis of the small
number of patients with subdiaphragmatic presentations who have been randomly
allocated either to radiation therapy or combined-modality treatment programs
that the prognoses of these patients are similar to those of supradiaphragmatic
early-stage patients [71]
[248]
[250]
[257]
; on the other hand, the prognosis for patients with intra-abdominal
presentations appears to be worse than that for patients with either
supradiaphragmatic presentations or peripheral subdiaphragmatic disease. [248]
This could be associated with age of patients, the presence of bulky masses, or
other factors. Krikorian et al. recommended clinical staging only, and treatment
with inverted Y plus splenic radiation, for patients with CS IA disease
presenting in the groin. [249]
For patients with CS IB, IIA, and IIB inguinal presentations, this group
recommended staging laparotomy and treatment with TNI including the mediastinum,
or combined-modality therapy, for those patients with PS IB or IIA disease. We,
on the other hand, believe that clinical staging should be adequate for all
peripheral subdiaphragmatic presentations. The only finding at laparotomy
resulting in upstaging is occult liver disease, which would be expected in fewer
than 5 percent of patients with CS IIA. Inverted Y plus splenic irradiation is
adequate therapy for patients with CS IA. Patients with CS IIA can be treated
with TNI therapy, and combination chemotherapy alone for patients with CS IIA is
also acceptable treatment. Patients with B symptoms have a high incidence of
extensive splenic involvement and hepatic involvement and should be treated with
combination chemotherapy. [250]
Therapy for patients with large abdominal masses should be individualized, but
should probably include both chemotherapy and involved-field radiation therapy
of the mass.
Stage IIIA
In this era, stage IIIA Hodgkin's disease should not be
considered early-stage disease and should not be treated with radiation therapy
alone. Although high CR rates (90 to 95 percent) are expected with TNI for stage
IIIA disease, [258]
[259]
between one third and two thirds of patients can be expected to relapse within 5
years. [260]
[261]
Retrospective studies in laparotomy-staged patients with PS IIIA disease have
identified two subsets with different prognoses following TNI, and these studies
have been used to justify laparotomy staging of these patients and treatment
with TNI alone in the better-prognosis subset. The first subgroup, termed PS III1
A, has subdiaphragmatic disease limited to lymphatic structures that accompany
the celiac axis group of arteries the spleen, splenic nodes, celiac nodes,
and/or portal nodes (disease limited to above the renal hila). PS III2
A involves the lower abdominal nodes para-aortic, iliac, or mesenteric nodes
(disease below the renal hila), with or without involvement of the spleen or the
upper abdominal nodes. Patients with PS III1 A had a
prognosis following radiation therapy similar to that of PS IIA patients,
whereas the second subgroup, PS III2 A, had a
significantly higher relapse rate. [260]
[261]
[262]
[263]
[264]
[265]
[266]
Relapse-free survivals at 5 years following TNI for PS III1
A and PS III2 A were 78 percent and 41 percent,
respectively, and the overall 5-year survivals were 93 percent and 57 percent,
respectively; these differences were significant. [261]
Although TNI and combined-modality therapy afforded similar CR rates and relapse
rates for patients with PS III1 A,combined-modality
therapy was significantly better than TNI for patients with PS III2
A. [266]
These trends were confirmed in a review of patients treated at four
institutions. [265]
On the other hand, retrospective analysis with much
longer follow-up duration of patients with PS III1 A
disease treated at the Joint Center for Radiation Therapy with either radiation
alone (STLI or TNI) or combined-modality therapy demonstrates a clear benefit,
not only in relapse-free survival, but also in overall survival, for patients
treated with combined-modality therapy, strongly suggesting that radiation
therapy alone is not sufficient therapy for either subclass of PS IIIA disease. [268]
Furthermore, both uncontrolled [159]
and controlled trials [240]
[269]
suggest that radiation therapy may not be necessary, since chemotherapy alone
and combined radiation therapy plus chemotherapy yield similar results for PS
IIIA. A randomized trial comparing MVPP with TNI demonstrated improved complete
remission rate and remission duration with combination chemotherapy. [270]
It should be noted that no randomized trial has demonstrated superior outcome
for patients treated with combined-modality therapy over those treated with
chemotherapy alone. We categorize stage IIIA disease as advanced-stage disease
and recommend chemotherapy alone for these patients. As a corollary, laparotomy
is never recommended for any CS III patient, since no germane information is
obtained.
Massive Mediastinal Disease
The most significant adverse prognostic factor in
otherwise early-stage Hodgkin's disease is massive mediastinal disease, and it
is now clear that, even when disease is found only above the diaphragm, disease
massively involving the mediastinum should be considered "advanced."
Most authors have used the straightforward definition of Mauch et al.: a
mediastinal mass is "massive" if the transverse diameter of the
mediastinal nodal mass is greater than one third of the widest diameter of the
thorax on a standing PA chest x-ray. [270]
The revised staging classification schema adopted at the Cotswolds conference [125]
recognized the poor prognosis of bulky disease by subclassifying all patients
with bulky disease with a subscript "X" following the anatomic stage,
and defined bulky mediastinal disease as greater than one third the diameter at
T5-T6.
As many as one quarter to one third of all newly
diagnosed patients with Hodgkin's disease and an estimated 15 to 20 percent of
those with stage I and II will have massive mediastinal disease. Nodular
sclerosis and mixed cellularity histologies comprise the bulk of patients with
mediastinal disease; LPHD virtually never involves the mediastinum massively.
Relapse rates for patients with stage II disease with large mediastinal masses
treated with radiation therapy alone have ranged between 50 and 74 percent. [213]
[272]
Mauch et al. found that patients of all stages with massive mediastinal disease
had higher relapse rates than comparably staged patients without massive
mediastinal disease, when treated with radiation therapy; in fact, stage I or II
patients with large mediastinal adenopathy had a higher relapse rate than did
patients with stage IV intrathoracic disease with small mediastinal involvement.
[271]
[273]
Half of PS IA and IIA patients with mediastinal masses greater than one third
the chest diameter treated with TNI relapsed, while only 2 percent of the
similarly treated patients without mediastinal masses and 12 percent of those
with small mediastinal masses relapsed; 8-year actuarial survivals were 86
percent and 96 percent, respectively, for large and small mediastinal masses.
Patients with stage IIE or stage IV massive mediastinal disease had a 64 percent
relapse-free survival and 66 percent overall survival at 5 years, compared with
90 percent relapse-free and 90 percent overall survival among stage IV patients
with small mediastinal masses. Most subsequent analyses have confirmed the
increased relapse rate in radiation therapy-treated patients with large
mediastinal masses, although not all have demonstrated significant survival
differences. [213]
[272]
[274]
[275]
[276]
[277]
[278]
[279]
[280]
[281]
[282]
[283]
[284]
[285]
An assessment of the results in massive mediastinal disease treated with
chemotherapy alone is difficult, since most of the comparatively few patients
who have been treated without radiation therapy have had stage IV disease, while
most of the patients treated with either radiation therapy alone or
combined-modality therapy have had anatomically limited disease. Retrospective
analysis of 49 patients with massive mediastinal disease treated at the NCI with
MOPP suggest that chemotherapy alone is not adequate
treatment for patients with stage III or IV disease. [286]
Ten of these patients received mantle field radiation therapy after MOPP
chemotherapy and the remainder received chemotherapy only. The complete response
rate among all these patients with bulky mediastinal disease was 71 percent and
the 20-year survival was 39 percent (cf., 84 percent CR rate and 48 percent
overall survival for all patients). [161]
The CR rate for the 39 patients treated with MOPP only was 67 percent with a 50
percent relapse rate, whereas 9 of the 10 treated with combined-modality therapy
entered CR with an 11 percent relapse rate. The overall survival of this small
group was higher at 20 years than was the survival of the group with massive
chest disease treated with MOPP only, but not significantly.
Because both radiation therapy alone and chemotherapy
alone have proven to be unsatisfactory when patients have bulky mediastinal
disease, most centers now routinely employ combined-modality therapy for this
subset of patients, irrespective of anatomic stage, using one of the
chemotherapy regimens described above for treatment of advanced disease, plus
mantle or involved field radiation therapy. A randomized trial comparing
radiation therapy alone and combined-modality therapy (MOPP plus mantle and para-aortic
irradiation) demonstrated significantly improved 10-year freedom-from-relapse
for patients treated with combined-modality therapy as compared with radiation
therapy (81 percent vs. 45 percent), although differences in overall survivals
were not significant. [213]
Other centers have subsequently reported salutary results with a combined
chemotherapy-radiation therapy approach to patients with large mediastinal
masses. [278]
[280]
[281]
[282]
[283]
[285]
[287]
The M.D. Anderson group has summarized its experience with combined-modality
therapy for massive mediastinal Hodgkin's disease with four different
chemotherapy regimens. [288]
Complete remission rates (CR, 85 percent overall), 3-year
freedom-from-progression (FFP, 76 percent overall), and 3-year
freedom-from-tumor-mortality (FTM, 90 percent overall) were similar among the
four regimens. The Stanford group has recently updated results of
combined-modality therapy with the Stanford V regimen (doxorubicin, vinblastine,
nitrogen mustard, vincristine, bleomycin, etoposide, and prednisone administered
over 12 weeks) followed by radiation therapy to a dose of 36 Gy to bulky sites
only. [230]
[289]
Forty-nine patients with massive mediastinal disease were included among a
larger group including patients with stages IIIB and IV, and although the
results for massive mediastinal patients were not reported separately, the
overall results were excellent: the 16-year actuarial overall survival and FFP
were 93 percent and 89 percent, respectively.
We have recently reported results of a prospective trial
in 80 patients with massive mediastinal disease using alternating MOPP-ABVD
chemotherapy followed by mantle field irradiation. [290]
The CR rate was 89 percent, and with median follow-up duration of 10 years, the
projected 15-year DFS for responders is 78 percent and overall survival at 15
years is 75 percent. Radiation treatment planning was performed before
chemotherapy was begun and following chemotherapy, 10 Gy radiation to mantle
field including the original full extent of disease was delivered, followed by
cone-down treatment to residual disease to a total dose of 35 to 45 Gy. This
regimen allows preservation of fertility more frequently and is associated with
a lower risk for leukemia than with MOPP, and is associated with a lower
incidence of pulmonary and/or cardiac toxicity than ABVD. Acute toxicities in
this trial were modest, though 21 percent of patients had some pulmonary
reaction within 3 months of completing therapy and 10 percent had cardiac
symptoms. One patient, an older patient with a history of heavy cigarette
smoking, died of lung toxicity. Three patients developed second malignancies.
Interestingly, no published studies have employed
combination chemotherapy alone in the treatment of patients with early-stage
disease accompanied by a large mediastinal mass. In our own early-stage
Hodgkin's disease trial, eight patients with massive mediastinal disease were
randomly assigned to receive MOPP alone before such patients were eliminated
from the study. All eight achieved a complete response and remain alive and in
their initial complete remission a median of 13 years after treatment. This
experience is certainly not large enough to suggest that radiation therapy can
be safely omitted in such patients. However, a large cooperative group study of
the need for radiation therapy in stage I and II massive mediastinal Hodgkin's
disease would be of interest.
Based on the above studies, we recommend treatment of
massive mediastinal Hodgkin's disease with combined-modality therapy,
irrespective of anatomic stage. Because laparotomy findings will not alter
treatment decisions, and because patients with bulky mediastinal masses are at
an increased risk of death during attempts to extubate following general
anesthesia, laparotomy staging should never be done in patients with massive
mediastinal HD. The alternating MOPP-ABVD regimen or the MOPP-ABV hybrid regimen
should be preferable to either MOPP or ABVD in this setting since the long-term
toxicities of both MOPP and ABVD may be increased by radiation exposure.
Chemotherapy should precede radiation therapy, since shrinking the tumor mass
before radiation allows significantly lower radiation dose to normal lung, and
initial chemotherapy allows earlier treatment to unirradiated sites. Although a
small dose of radiation was delivered to the original tumor volume in the NCI
trial described above, [290]
including a large volume of normal lung in the initial treatment field in many
patients, it is not clear that this practice is necessary.
Stage III and IV Disease
The treatment for advanced-stage Hodgkin's disease has
advanced very little in the last 20 years. The choice of chemotherapy regimen
has been discussed above. ABVD alone, ChlVPP, MVPP or MOPP alone, MOPP
alternating with ABVD, or one of the hybrid regimens MA/MA or MOPP/ABV are all
reasonable choices. ABVD has pulmonary and cardiac toxicities as its only
drawbacks
2644
and is the first choice in practice today. About 10 percent of patients
receiving any of these regimens will have persistent radiographic abnormalities
or persistent positive gallium scans after six cycles of therapy. If the
residual disease has improved between cycles four and six, two additional cycles
of chemotherapy may be given. However, the most effective method of converting
such patients to complete responders is probably the addition of involved field
radiation therapy to the residual sites of disease. In the vast majority of
cases, patients can be converted to complete responders with this approach.
Efforts to improve upon the outcome of chemotherapy alone
in advanced-stage patients are based on the success of high-dose therapy and
autologous stem cell support in the treatment of relapsed patients. It has been
difficult to justify high-dose therapy as a primary treatment approach because
no subsets of patients appeared to have a sufficiently poor prognosis with
combination chemotherapy that high-dose therapy was warranted. Two approaches
have been taken; development of a more effective conventional-dose regimen and
development of a prognostic factor model to identify high-risk patients.
Stanford V, alluded to above, consists of seven drugs given in alternating
combinations weekly for 12 weeks. The BEACOPP (carmustine, etoposide, cytarabine,
cyclophosphamide, vincristine, prednisone, and procarbazine) regimen [291]
was dose-escalated by increasing the doses of etoposide, doxorubicin, and
cyclophosphamide and administering together with granulocyte colony-stimulating
factor (G-CSF) in 3-week cycles. Preliminary analysis of escalated BEACOPP
versus COPP/ABVD appears to favor BEACOPP. The regimen might be even more
effective if given to patients with advanced-stage disease with clinical
features suggesting a poorer prognosis. Both the Stanford V and BEACOPP regimens
were followed by involved field radiation therapy; there remains no controlled
data to support that practice.
Recently, an international collaboration set out to
define prognostic subsets within patients with advanced-stage disease treated
with the most effective combination chemotherapy programs. Twenty-five centers
from all over the world pooled their data on patients with advanced-stage
disease for analysis. The result is a new International Prognostic Factor Index
for advanced Hodgkin's disease. The following seven clinical factors emerged as
having prognostic relevance: serum albumin less than 4 g/dl, hemoglobin less
than 10.5 g/dl, male gender, stage IV disease, age older than 45 years, white
blood cell count greater than 15,000/mm3 , and
lymphocyte count less than 600/mm3 . Each factor
exerted roughly an equivalent effect on freedom from progression, about 8
percent. The results are summarized in Table 90-7 .
For the purposes of clinical studies, it is convenient to divide patients into
two groups: patients with 0 to 2 factors comprise about 58 percent of all
advanced-stage patients and have a freedom from progression at 5 years of about
74 percent; patients with three or more factors comprise about 42 percent of all
advanced-stage patients and have a freedom from
progression at 5 years of 55 percent. Efforts to intensify the therapy for the
latter group may well lead to improved outcome in advanced disease. [292]
Relapsed and Refractory Disease
Relapse after radiation
Chemotherapy has been shown to be excellent salvage
therapy for the 20 to 25 percent of patients treated initially with radiation
therapy who relapse. [160]
[292]
[293]
[294]
[295]
It appears that any of the front-line chemotherapy regimens previously discussed
is capable of curing patients who relapse after radiation therapy, with expected
complete remission rates between 75 and 90 percent and long-term survival after
relapse ranging between 45 and 70 percent. An analysis of prognostic factors in
109 patients treated with MOPP or MOPP-like chemotherapy at Stanford University
after relapse from radiation therapy [297]
suggests that extent of disease at the time of relapse, as measured by anatomic
stage at relapse (termed relapse stage [RS]) is the most important factor
predicting second CR, freedom from second relapse (FF2ndR), and overall survival
after first relapse. For the overall group with median follow-up of 8.3 years,
the 10-year FF2ndR was 57 percent. The 10-year FF2ndR rate for 26 patients with
RS IA was 90 percent; for 34 patients with RS IIA and IIIA, 60 percent; and for
49 patients with IB, IIB, IIIB, and IV the FF2ndR rate was 30 percent. Age
greater than 50 years was the only
*Data from Hoppe RT, Coleman CN, Cox RS, et al:
The management of stage I-II Hodgkin's disease with irradiation alone or
combined modality therapy: the Stanford experience. Blood 59:455, 1982.
*Data from Hasenclever D, Diehl V, for the
International Prognostic Factors Project on Advanced Hodgkin's Disease: a
prognostic score for advanced Hodgkin's disease. N Engl J Med 339:1506, 1998.
other negative predictor of outcome at relapse. This suggests that the primary
reason that the overall long-term results following chemotherapy salvage for
patients relapsing after radiation therapy have appeared to be somewhat better
than those for advanced-stage patients treated initially with chemotherapy is
that these relapses tend to be identified at an early stage due to careful
follow-up; stage-for-stage, treatment of relapse after radiation therapy appears
to yield somewhat worse results than are observed with de novo treatment.
Relapse after chemotherapy
The likelihood of response to salvage therapy and
long-term prognosis of patients relapsing after initial chemotherapy depend on,
among other prognostic variables, the response to initial therapy and duration
of the first remission, segregating those who are not cured by their initial
therapy into three groups: (1) induction failures patients who never enter
complete remission; (2) relapse less than 12 months after achieving complete
remission; and (3) relapse greater than 12 months after achieving complete
remission. Median survival from date of relapse for each group is 1.3, 2.6, and
4.3 years, respectively. [298]
The last group of patients is recognized to have an excellent response to
salvage chemotherapy, whether the same regimen as the first-line regimen or a
different regimen is used, whereas the
first two groups of patients fare considerably less well. Analysis of the NCI
experience with patients relapsing after chemotherapy suggests that even those
patients whose initial remission was longer than 12 months and who achieve
second complete remissions have a very low probability of being cured by
conventional-dose salvage therapy. [298]
Of a total of 439 patients treated with MOPP or a related regimen between 1964
and 1990, 107 relapsed after achieving complete remission (approximately half of
these relapses occurred <1 year after first CR). The overall survival of all
relapsed patients is projected to be 17 percent at 20 years. Both the
probability of achieving a second complete response and the overall survival
were predicted by the duration of the first remission. Response rate and
survival were not significantly affected by initial stage or symptoms or initial
chemotherapy regimen. Second CR rate for patients whose initial complete
remission was longer than 12 months, most of whom were retreated with MOPP, was
79 percent; whereas for patients with initial remission durations less than 12
months (62 percent of whom were treated with regimens other than MOPP), the
second remission rate was 49 percent. Second remissions were significantly more
durable for patients with long initial remissions than for those with initial
remissions less than 1 year: 45 percent actuarial 22-year disease-free survival
for patients achieving second complete remission after a long initial remission
compared with 14 percent 5-year disease-free survival for patients with first
relapse after less than 1 year. Due largely to deaths from acute leukemias and
other treatment-related complications, the overall survival was unfortunately
only 24 percent for those patients with long first remissions and 11 percent for
those whose first remissions were less than 12 months.
The ABVD regimen was designed specifically to treat MOPP-resistant
patients. [186]
An early report found a 59 percent CR rate in 55 patients with MOPP-resistant
Hodgkin's disease treated with ABVD salvage therapy. [299]
No correlation between response rate and duration of MOPP response was noted; in
fact, complete remission was obtained in 52 percent of 29 patients who had
progressive disease during MOPP chemotherapy. About two thirds of the responders
relapsed, leading the authors to conclude that ABVD "can probably cure one
third of complete responders and therefore about 20 percent of all MOPP-resistant
patients." [299]
Other groups employing ABVD or similar doxorubicin-containing salvage regimens
have not been able to duplicate these results, with CR rates generally ranging
between 10 and 45 percent. [300]
[301]
[302]
[303]
[304]
[305]
[306]
[307]
[308]
[309]
[310]
Indeed, in the aforementioned CALGB study, patients randomly assigned to MOPP or
ABVD were crossed over to the other four-drug regimen upon relapse;
interestingly, MOPP was significantly more effective at rescuing ABVD treatment
failures than was ABVD at rescuing MOPP treatment failures.
One retrospective analysis of the outcome of salvage
therapy for first relapse following MOPP or a MOPP-like regimen suggests that
the outcome is highly dependent on the presence of three risk factors symptoms
2646
at the time of relapse, time to relapse of less than 1 year, or stage IV disease
at original diagnosis and is rather less dependent on the type of the salvage
treatment. [311]
The presence of any one of three risk factors predicted a 5-year
freedom-from-second-failure ([FF2F] defined as failure to achieve second CR,
toxic death, or relapse after a second CR) of 17 percent, irrespective of
salvage therapy (including high-dose salvage with ABMT at first relapse!),
whereas the absence of these risk factors predicted a 5-year FF2F of 82 percent.
Patients without risk factors treated with extended field irradiation or with
doxorubicin-based chemotherapy (MOPP-ABVD or MOPP-ABV) had a 100 percent 5-year
FF2F; patients lacking risk factors treated with high-dose chemotherapy and ABMT
had a 75 percent 3-year FF2F; while patients salvaged with MOPP had a 40 percent
5-year FF2F. (With much shorter follow-up, this 5-year result with MOPP salvage
is probably comparable to the 24 percent 20-year overall survival reported from
the NCI for a group of patients relapsing >1 year after MOPP but including
patients with the other two risk factors. [298]
) The main problem in interpreting this retrospective study is that in each risk
factor and salvage therapy category, the total number of patients is very small,
making statistical comparisons underpowered.
Clearly, many relapsed patients have complete remissions
and prolonged disease-free intervals with conventional salvage therapy.
Re-treatment with MOPP or salvage with a doxorubicin-containing regimen is very
good reinduction therapy for patients whose initial remission is greater than 1
year, while ABVD or one of its derivatives appears to be a better choice for
patients whose first remission is less than 1 year (unless ABVD was part of the
initial treatment). An alkylating agent-containing regimen (ChlVPP or MOPP) is
effective in patients who relapse after ABVD treatment. Extended field radiation
therapy may be considered for low-risk patients relapsing with limited disease
at the time of relapse. However, even for the group of patients lacking putative
risk factors, there is a low probability of cure with conventional salvage
chemotherapy, and most of these patients will, at some point in the course of
their subsequent treatment, be candidates for a high-dose salvage regimen. For
patients relapsing after less than 1 year, or those with one of the other
high-risk factors mentioned above, high-dose therapy with ABMT may be considered
following re-induction with conventional-dose salvage therapy, with the caveats
discussed below. [311]
Patients who do not achieve a complete remission with
initial therapy, who have first complete remissions lasting less than 1 year, or
who are in second or subsequent relapse are generally considered candidates for
high-dose salvage regimens with either autologous bone marrow transplant (ABMT)
or autologous peripheral blood stem cell transfusions (APBSCT). [312]
[313]
[314]
The drugs used in these programs have myelosuppression as the primary
dose-limiting toxicity and are used in doses above the lethal dose to bone
marrow in the absence of stem cell re-infusion, but below the limit of
life-threatening nonhematologic toxicity. The most commonly used regimens are
BEAM (BCNU, etoposide, cytarabine, and melphalan) and CBV (cyclophosphamide,
BCNU, and etoposide). Initial debulking with conventional-dose regimens before
ablative therapy increases the effectiveness of the high-dose therapy, and
several intensive salvage programs for initial debulking, generally including
hematopoietic growth factor support, have been developed. These include MINE (mitoguazone,
ifosfamide, navelbine, and etoposide), [315]
dexa-BEAM, [316]
mini-BEAM, [317]
and EPOCH (etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin).
[318]
About 35 to 45 percent of the highly selected patients
treated in various reported trials have prolonged disease-free survival
following high-dose salvage therapy and, because of perceived superiority over
conventional salvage programs, this approach has become standard treatment,
unfortunately without the proof of benefit afforded by large randomized clinical
trials. Critical assessment of the overall benefit or the optimal timing of
high-dose salvage therapy is difficult. The selection process for high-dose
therapy favors younger patients with good performance status and little or no
end-organ damage (i.e., the same patients who would be expected to do well with
conventional salvage therapy). One randomized trial was attempted by the British
National Lymphoma Investigation, comparing high-dose BEAM with ABMT versus
mini-BEAM. Early results suggested that high-dose BEAM was better than
mini-BEAM, but accrual was stopped after only 40 patients were randomized, and
before proof of benefit could be obtained, because physicians refused further
participation. [319]
Toxicity of ablative regimens is, of course, a major
concern. High rates of infection occur during the 3 weeks or so required for
marrow engraftment and production of adequate levels of neutrophils. The
mortality rate in most of the reported trials averages 5 to 10 percent and
somewhat higher when the preparative regimen includes radiation. Interstitial
pneumonitis is the cause of one half to two thirds of the treatment-related
deaths, followed by bacterial or fungal sepsis and cardiac failure. Although no
prospective study that would allow a judgment about optimal timing of high-dose
salvage therapy has been performed, theoretical considerations suggest that
using high-dose therapy earlier in the course of relapsed disease rather than
later would be advantageous [320]
: significant decreases in morbidity and mortality should be realized by
employing high-dose salvage before damage to marrow and other organs caused by
multiple previous chemotherapy salvage regimens and radiation therapy
accumulates; furthermore, tumor burden at the time of treatment is more likely
to be low and, consequently, the likelihood of encountering biochemical
resistance to the drugs should be lower. Experience in 22 high-risk patients in
first remission following alternating MOPP-ABVD, then treated with CBV and ABMT,
has been reported. [321]
Seventeen of the patients (77 percent) were alive and continuously in CR at a
median of 86 months following ABMT, with an actuarial overall survival of 80
percent. A group of 24 patients said to have similar risk factors at the time of
diagnosis, who refused high-dose therapy, were offered as a control. Sixteen of
these patients died of relapsed HD, with only 33 percent alive and free of HD at
a median of 89 months after their last course of MOPP-ABVD. It is, of course,
not possible to determine from this small, nonrandomized study whether the
reported results are truly better than could be expected from conventional-dose
therapy.
For patients whose initial remission was longer than 12
months, the evidence is good that conventional-dose salvage chemotherapy is able
to induce second remissions in the majority of patients. However, the durability
of remissions is usually poor. For that reason, some investigators have also
used high-dose therapy with autologous bone marrow or stem cell transplantation
in the relapsed patients with better prognosis. Reece and colleagues reported
long-term disease-free survival in 79 percent of such patients, a result that is
much better than would be expected from conventional-dose salvage therapy. [322]
Therefore, it is reasonable to consider high-dose therapy for any patient not
cured with their initial course of combination chemotherapy.
Late Complications of Therapy
As has been mentioned throughout this chapter, prolonged
survival following effective therapy for Hodgkin's disease has been accompanied
by several late sequelae, notably second malignancies, gonadal toxicity,
hypothyroidism, and heart and lung toxicities. [323]
[324]
In a large epidemiologic study from the Netherlands Cancer Institute of 1,984
patients treated for Hodgkin's disease between 1966 and 1986, the cumulative
risk of death at 20 years from diagnosis was 33 percent from HD or acute
treatment toxicity, 14 percent from second malignancies, and 20 percent from all
other causes, the most important of which was cardiovascular disease. [325]
The risk of dying from second malignancies and other treatment-related causes
continued to increase even after 20 years' follow-up. Awareness of the risks of
these late toxicities is essential during initial treatment planning and during
the lifelong follow-up period following treatment. When therapies of equal
curative potential have different toxicities, the risk for potential late
complications should guide choice of therapy. If an inherently increased risk of
a treatment-related complication can be exacerbated by patient behavior, as is
the case for the association of cigarette smoking with lung cancer following
radiation therapy to the lungs, the patient at risk must be emphatically urged
to eliminate the risky behavior. The physician must periodically reassess for
the occurrence of late-appearing side effects and, in some cases, institute
routine screening when early detection and treatment may make a difference, as
is the case with radiation-induced breast cancer. Finally, we must not forget
the truism that a prerequisite for susceptibility to death of a late
complication of treatment 15 to 25 years after diagnosis of Hodgkin's disease is
successful initial therapy.
Myeloid Malignancies
Cases of secondary myeloid malignancy, including
myelodysplastic syndrome (MDS) and acute nonlymphocytic leukemia (ANLL) occur
between 2 and 10 years following completion of therapy for Hodgkin's disease
that includes alkylators, especially nitrogen mustard, chlorambucil,
nitrosoureas, and procarbazine; thereafter, the incidence returns to that of the
untreated population. Antileukemic chemotherapy for secondary ANLL seldom yields
long-term remissions, and death within 4 to 8 months is usual. Multiple
cytogenetic abnormalities, especially involving chromosomes 5 and 7, are
characteristic of secondary myeloid leukemias. [326]
[327]
[328]
The cumulative risk of secondary leukemia and
myelodysplastic syndrome for patients in first remission after six to eight
cycles of MOPP or similar alkylator-containing chemotherapy without radiation
therapy or maintenance therapy is 1.5 to 3 percent at 10 years and there is a
dose-related increase in leukemia risk with increasing alkylator exposure and
number of total treatment cycles. Thus, it is especially important to avoid
exposures to alkylating agents that have been shown to be ineffective, such as
maintenance chemotherapy after remission induction. The risk of myeloid
malignancy after ABVD alone is nil. An epidemiologic study from the Netherlands
Cancer Institute demonstrates clearly a lower incidence of leukemia/MDS in
patients treated in the 1980s as compared with those treated in the 1970s, due
to wide use of the MOPP/ABVD combination in the 1980s. [325]
Evidence from several epidemiologic studies suggests that splenectomy increases
the risk for leukemia. [325]
[329]
[330]
Although several earlier reports suggested synergy between radiation therapy and
alkylator therapy in causing myeloid malignancies, [161]
[331]
[332]
[333]
recent epidemiologic studies have suggested that radiation therapy adds little
or no additional risk to alkylator-containing chemotherapy. [325]
[334]
[335]
[336]
The increased risk from radiation therapy is probably associated with larger
field size and higher doses.
Non-Hodgkin's Lymphomas
Long-term Hodgkin's disease survivors are at increased
risk for B-cell non-Hodgkin's lymphomas, usually of intermediate to high
histologic grade. [325]
[332]
[335]
[337]
[338]
[339]
[340]
[341]
These lymphomas have a propensity for extranodal presentation, particularly in
the gastrointestinal tract with a predilection for the ileocecal valve, not
infrequently presenting with abdominal pain due to intussusception of the mass.
Secondary lymphomas generally respond well to therapy that is effective in
sporadic cases of aggressive lymphoma.
The similarity between the presentation of these
lymphomas and non-Hodgkin's lymphomas that occur with high frequency in
immunodeficiency states such as organ transplants or AIDS has suggested to many
observers that non-Hodgkin's lymphoma is a consequence not of direct
lymphomagenicity of the treatment itself but rather of a residual
immunodeficiency
2648
associated with the Hodgkin's disease, perhaps exacerbated by therapy. [337]
This view is contradicted by a recent study that found at least in part an
association with previous therapy, the risk being lowest in patients treated
with radiation alone and highest among patients treated with intensive
combined-modality programs. [325]
Solid Tumors
Most of the excess risk of dying in Hodgkin's disease
patients greater than 10 years after treatment is from solid tumors occurring
within the field of previous radiation. Estimates of cumulative risk for solid
tumors range from 8 to 13 percent at 15 years [333]
[335]
[342]
to as high as 24 percent at 24 years in a cohort of pediatric patients. [329]
Lung cancer is the most frequent second solid tumor, followed by stomach cancer,
melanoma, and soft tissue sarcomas. [335]
Lung cancer occurs almost exclusively in patients who smoked cigarettes, but at
a much higher incidence than in nonirradiated smokers. Other tumors occurring
with a greater than expected frequency include breast cancer, thyroid cancer
(67-fold relative risk for children with Hodgkin's disease irradiated to the
neck), bladder carcinoma, and head and neck cancer. [343]
[344]
An increased risk for breast cancer following mantle
field radiation therapy has been firmly established. [325]
[345]
Among 885 women treated with radiation therapy at Stanford University followed
for a median of 10 years, 25 developed breast cancer, in comparison with about
six cases expected in age-matched controls, for a relative risk (RR) of 4.1. The
risk of developing breast cancer was highly dependent on the age at irradiation:
for girls treated before age 15, the RR was 136; for those 15 to 24, RR was 19;
and for those 24 to 29, RR was 7. The risk was not increased for women treated
after age 30. The average interval from treatment to the diagnosis of breast
cancer was 15 years, and the risk increased significantly with follow-up time
greater than 15 years. A further increased risk was detected in women who had
been treated with both MOPP and radiation therapy, although it was thought that
estrogen-replacement therapy following iatrogenic menopause may have contributed
to this risk. The actuarial and disease-free survivals following breast cancer
diagnosis were slightly lower than expected for breast cancer in the general
population. Both the finding of an elevated risk for breast cancer limited to
women who were irradiated before age 30 and the 15-year latency before increased
risk could be detected were corroborated in the large epidemiologic study from
the Netherlands. [325]
A clinical analysis of 37 women with Hodgkin's disease
and subsequent breast cancer (from an undefined population at risk) was
reported. [346]
[347]
All patients had received radiation therapy to the mediastinum, 80 percent to a
dose greater than 35 Gy. The median age at diagnosis of breast cancer in these
women was 43 years with a median interval since treatment of Hodgkin's disease
of 15 years; 68 percent of the patients had been treated for Hodgkin's before
age 30. Eight patients (22 percent) developed bilateral breast cancer. In
comparison with breast cancer patients from the general population, there was an
increased propensity for presentation in the medial half of the breast (the
portion with the greatest radiation exposure). The prognosis of these patients
was strongly dependent on the axillary nodal status; survival in both
node-negative and node-positive categories was similar to the survival in
comparable primary breast cancer patients. Findings were positive in 81 percent
of 32 mammograms of involved breasts available for review. Although it was not
stated what prompted the mammographic studies (i.e., whether the mammograms were
obtained for screening or after identification of palpable breast masses or
other symptoms), a previous analysis of 29 (90 percent positive) of these
mammograms had shown that in 15 of the 29 tumors (52 percent), both physical
examination and mammography were positive; in 11 (38 percent), mammography was
positive while physical exam was negative; whereas, in three (10 percent), the
mammogram was negative and physical exam was positive. [347]
Based on the data in these studies, we recommend routine
screening for breast cancer for all women who receive radiation to mediastinal
or mantle fields for Hodgkin's disease before age 30 beginning 8 to 10 years
after completion of radiation therapy, to include yearly breast examination and
mammography.
Gonadal Failure
Sterility following chemotherapy, especially MOPP, or
direct radiation therapy to the gonads, can be an important sequela of
treatment. [348]
[349]
[350]
The risk of sterility in men or women is nil following treatment with ABVD. [206]
Virtually 100 percent of males have azoospermia immediately following a course
of therapy with MOPP, and fewer than 10 percent will recovery normal sperm
counts 6 months to 4 years after completion of chemotherapy. [351]
Potency is not affected. The risk for sterility following MOPP in women
increases with age of treatment. Affected women experience premature menopause
due to injury to the rapidly dividing follicular epithelial cells of the ovary. [348]
[352]
[353]
Some of the menopausal symptoms can be misattributed to recurrence of Hodgkin's
disease and can provoke unnecessary testing, even including laparotomy. In the
NCI series 89 percent of women who were older than 25 at the time of therapy
became amenorrheic, whereas only 20 percent of the women who were younger than
25 at the time of treatment experienced menopause. [354]
The onset of amenorrhea occurred less than 1 year after the completion of
therapy in women older than 31. Women treated with MOPP before age 30 who
underwent menopause frequently noted a gradual decrease in frequency of menses
over several years, accompanied by perimenopausal hormone levels, culminating
invariably in menopause. In the Stanford series [355]
a sigmoidal increase in probability of ovarian failure with age was noted, with
less than 50 percent probability of retaining regular cyclic menses when
treatment was given after age 25. Even in women who
regain their menses after MOPP therapy, most undergo menopause earlier than
normal.
If fertility is a concern for either men or women with
Hodgkin's disease for whom chemotherapy is indicated, consideration should be
given to the use of ABVD instead of MOPP. It appears that three cycles of MOPP,
as would be given in the MOPP-ABVD alternating regimen, probably is the limit of
exposure that will allow recovery of spermatogenesis in about half of treated
men. If MOPP chemotherapy is planned, or if testicular radiation is necessary,
sperm banking can be considered for men who desire to father children. In
general, men with Hodgkin's disease have oligospermia related to the disease
even before the onset of treatment. However, pregnancy following artificial
insemination can be successful even for men with oligospermia before therapy,
although the success rate of this procedure may be lower than for the normal
population.
Late Cardiac and Pulmonary Toxicity
Depending on the radiation therapy techniques used and on
the amount of intrathoracic tumor, mediastinal irradiation can result in an
increased incidence among long-term survivors of Hodgkin's disease of
constrictive pericardial disease, cardiomyopathy, and radiation pneumonitis and
fibrosis. [356]
These sequelae can be exacerbated by doxorubicin and bleomycin. Many of these
late side effects have been greatly decreased due to refinement of radiation
therapy techniques, [357]
[358]
but radiation therapy to the entire cardiac volume still results in significant
reductions in left ventricular function. [359]
Furthermore, a recent reassessment of patients treated with radiation therapy
for Hodgkin's disease at Stanford has revealed a substantial 3.2-fold relative
risk for death from myocardial infarction over 20 years among patients treated
with radiation therapy as compared with an age- and sex-matched normal
population. [155]
The long-term risk for heart and lung toxicity among patients treated with ABVD
or a related regimen without radiation therapy has not been carefully assessed.
However, bleomycin in other regimens [360]
has been associated with late toxicity and the report of toxicity in the CALGB
comparative study [194]
suggests that acute and chronic pulmonary toxicity and heart failure may be
serious problems following ABVD.
Infections
Patients who have been treated for Hodgkin's disease
generally have readily measurable defects in the function of their T cells, and
some evidence suggests that these defects may be present even before the onset
of Hodgkin's disease. Thus, patients with Hodgkin's disease have some immune
compromise that is not necessarily a consequence of the treatment. In general,
the immune compromise does not lead to frequent infections; however, infections
are the third leading cause of death in patients cured of Hodgkin's disease
behind heart disease and second cancers. [361]
Patients without spleens are at the greatest risk. Prophylactic antibiotics have
not been shown to be effective and pneumococcal vaccine is only partially
protective after splenectomy. Thus, patients require education regarding the
importance of seeking medical attention promptly if they develop symptoms of
fever or signs of infection.